The Child-Pugh score is one of the most widely used systems for classifying the severity of chronic liver disease. It combines three biochemical markers of hepatic function with two clinical assessments of complications, producing a total score that stratifies patients into Classes A, B, and C — from well-compensated to decompensated cirrhosis.
Despite being over 50 years old, the Child-Pugh classification remains a cornerstone of hepatological practice, informing prognosis, guiding decisions about surgical risk, procedural suitability, and the need for liver transplant evaluation. Understanding how it is scored, what each component measures, and where its limitations lie is essential for any doctor managing patients with liver disease.
The Child-Pugh score is a clinical scoring system used to classify the severity of cirrhosis. It combines bilirubin, albumin, INR, ascites, and hepatic encephalopathy to produce a total score from 5 to 15, classifying patients into Child-Pugh Classes A, B, or C. Class A represents compensated cirrhosis; Class C represents advanced decompensated disease.
Learning Objectives
- Describe the historical development of the Child-Pugh score
- List the five components of the Child-Pugh score and score each parameter
- Calculate a Child-Pugh score from given clinical and biochemical data
- Interpret Child-Pugh Classes A, B, and C with associated prognosis
- Identify the clinical uses of the Child-Pugh score
- Recognise the limitations of the Child-Pugh score and how MELD addresses them
Historical Background
The Child-Pugh score has its origins in work by CG Child and JG Turcotte in 1964, who proposed a classification system for predicting operative mortality in patients with cirrhosis undergoing portosystemic shunt surgery. Their original score included bilirubin, albumin, prothrombin time, ascites, encephalopathy, and nutritional status, divided into three classes (A, B, C).
In 1973, Roger Williams and RNH Pugh modified this system by replacing the nutritional status parameter (which was difficult to standardise) with a more precise prothrombin time measurement. The result was the Child-Pugh score as it is used today — five parameters, each scored 1–3, giving a total out of 15.
Why Liver Severity Scoring is Needed
The liver has enormous functional reserve. Patients with cirrhosis can appear clinically well (compensated cirrhosis) with relatively preserved synthetic function and no complications. Others with the same histological diagnosis may be profoundly unwell with jaundice, ascites, coagulopathy, and encephalopathy (decompensated cirrhosis).
A standardised scoring system allows clinicians to:
- Communicate severity consistently between teams and institutions
- Predict short- and medium-term mortality
- Risk-stratify patients before surgery or interventional procedures
- Determine eligibility and priority for liver transplantation evaluation
- Guide decisions about appropriateness of certain medications and dose adjustments
The Five Components
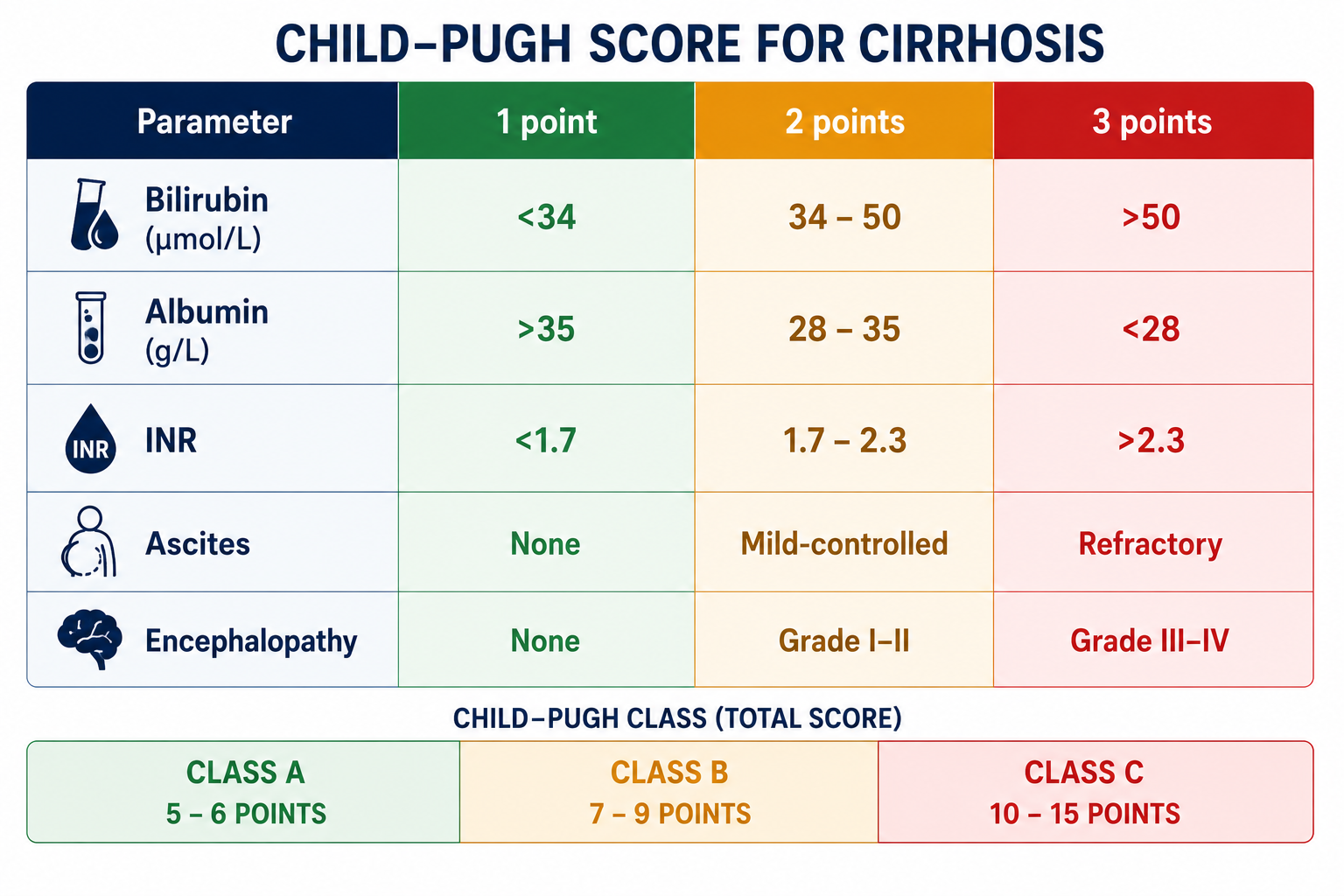
The Child-Pugh score uses five parameters. Three are objective laboratory values; two are clinical assessments. Each is scored 1, 2, or 3:
| Parameter | 1 Point | 2 Points | 3 Points |
|---|---|---|---|
| Bilirubin (μmol/L) | <34 | 34–50 | >50 |
| Albumin (g/L) | >35 | 28–35 | <28 |
| INR | <1.7 | 1.7–2.3 | >2.3 |
| Ascites | None | Mild / controlled with diuretics | Moderate / refractory |
| Hepatic Encephalopathy | None | Grade I–II (mild/moderate) | Grade III–IV (severe/coma) |
The thresholds above use SI units (μmol/L). Some resources quote thresholds in mg/dL: <2 mg/dL = 1 point, 2–3 mg/dL = 2 points, >3 mg/dL = 3 points. To convert: 1 mg/dL ≈ 17.1 μmol/L.
Understanding Each Parameter
Bilirubin reflects the liver's ability to conjugate and excrete bile. In hepatocellular disease, failure of conjugation raises unconjugated bilirubin; in cholestatic disease (e.g. PBC, PSC), failure of excretion raises conjugated bilirubin. Either way, hyperbilirubinaemia reflects hepatic dysfunction.
Albumin is synthesised exclusively by the liver and has a half-life of approximately 20 days. It is therefore a marker of chronic hepatic synthetic function — a low albumin in a patient without protein malnutrition or nephrotic syndrome suggests long-standing hepatic impairment. Note: albumin is an acute phase reactant and falls in sepsis/inflammation; this may confound interpretation in acutely unwell patients.
INR reflects acute hepatic synthetic function — specifically the production of Factors I, II, V, VII, and X. Factor VII has the shortest half-life (~4–6 hours), so INR responds rapidly to changes in hepatic function. A rising INR is an early and sensitive sign of hepatic decompensation. For a full explanation of why INR is used here, see PT and INR Explained.
The original Child-Turcotte classification used PT prolongation rather than INR. Modern practice uses INR because it standardises coagulation assessment between laboratories. INR removes variation caused by differences in thromboplastin reagents and allows more reliable comparison of hepatic synthetic function across institutions. For a detailed explanation of the difference, see PT and INR Explained and How INR Is Calculated.
Ascites results from portal hypertension, hypoalbuminaemia, and neurohormonal changes (RAAS activation, ADH release) that promote sodium and water retention. The development of ascites marks a major transition from compensated to decompensated cirrhosis and significantly worsens prognosis.
Hepatic encephalopathy (HE) is a neuropsychiatric complication of hepatic failure caused by accumulation of toxins (especially ammonia) that the failing liver cannot clear. It ranges from subtle personality changes (Grade I) to coma (Grade IV). Overt HE is one of the most distressing and prognostically significant complications of cirrhosis.
Worked Example
The best way to understand the Child-Pugh score is to calculate it from real clinical data. Consider the following patient with cirrhosis:
| Parameter | Patient Value | Score | Reason |
|---|---|---|---|
| Bilirubin | 42 μmol/L | 2 | 34–50 μmol/L → 2 points |
| Albumin | 31 g/L | 2 | 28–35 g/L → 2 points |
| INR | 1.8 | 2 | 1.7–2.3 → 2 points |
| Ascites | Mild, controlled with diuretics | 2 | Mild/controlled → 2 points |
| Hepatic Encephalopathy | None | 1 | None → 1 point |
| Total Score | 2 + 2 + 2 + 2 + 1 = 9 | ||
A total Child-Pugh score of 9 falls within the range 7–9, corresponding to Child-Pugh Class B — significant functional compromise with intermediate prognosis. This patient has mild hepatic decompensation with controlled ascites and moderately impaired synthetic function.
In examinations, always score each of the five parameters individually before assigning the final Child-Pugh class. Do not attempt to estimate the class directly from the clinical picture. A systematic parameter-by-parameter approach avoids errors and demonstrates correct method.
Child-Pugh Classes
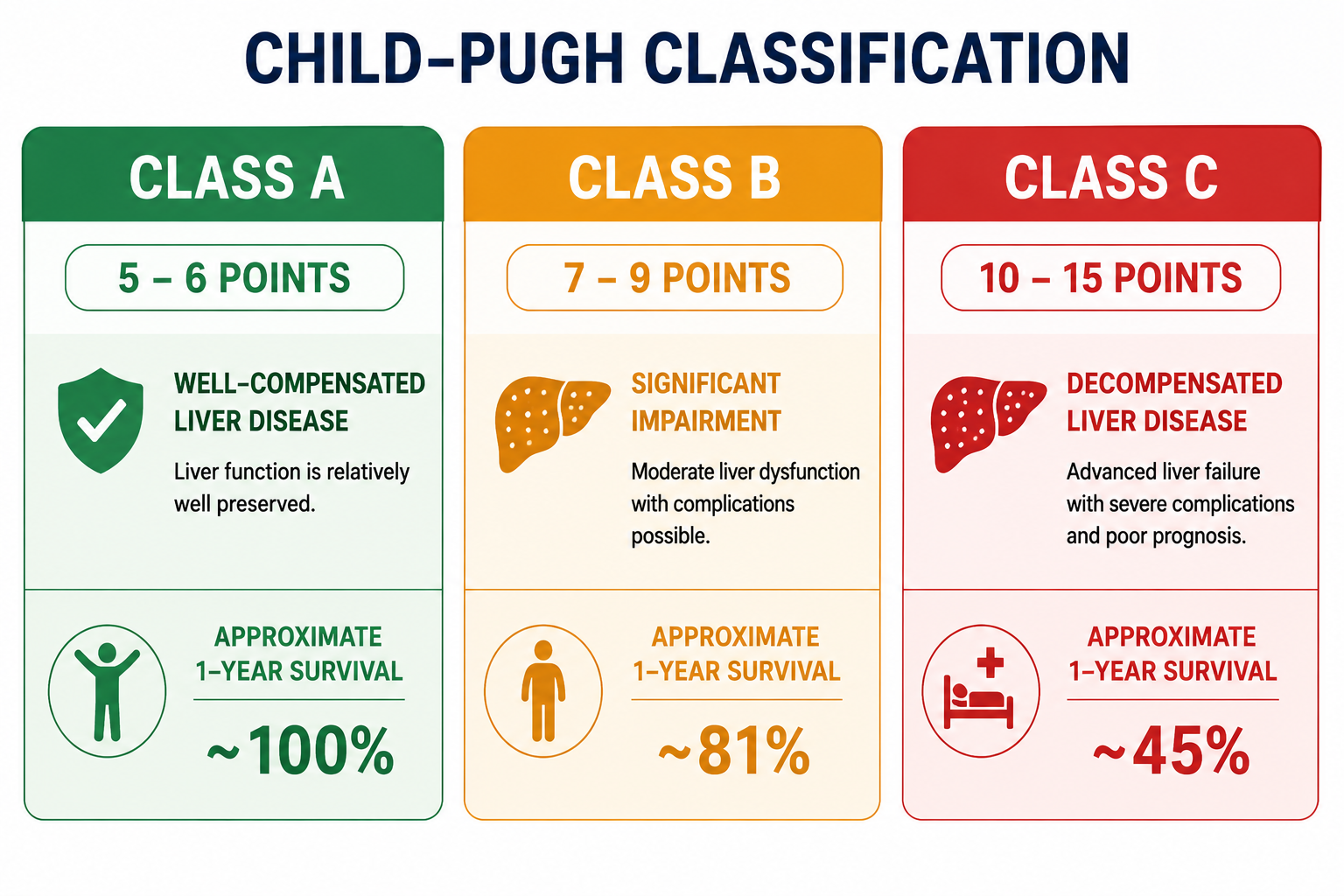
| Class | Total Score | Description | 1-Year Survival | 2-Year Survival |
|---|---|---|---|---|
| A | 5–6 | Well-compensated cirrhosis | ~100% | ~85% |
| B | 7–9 | Significant functional compromise | ~81% | ~57% |
| C | 10–15 | Decompensated cirrhosis | ~45% | ~35% |
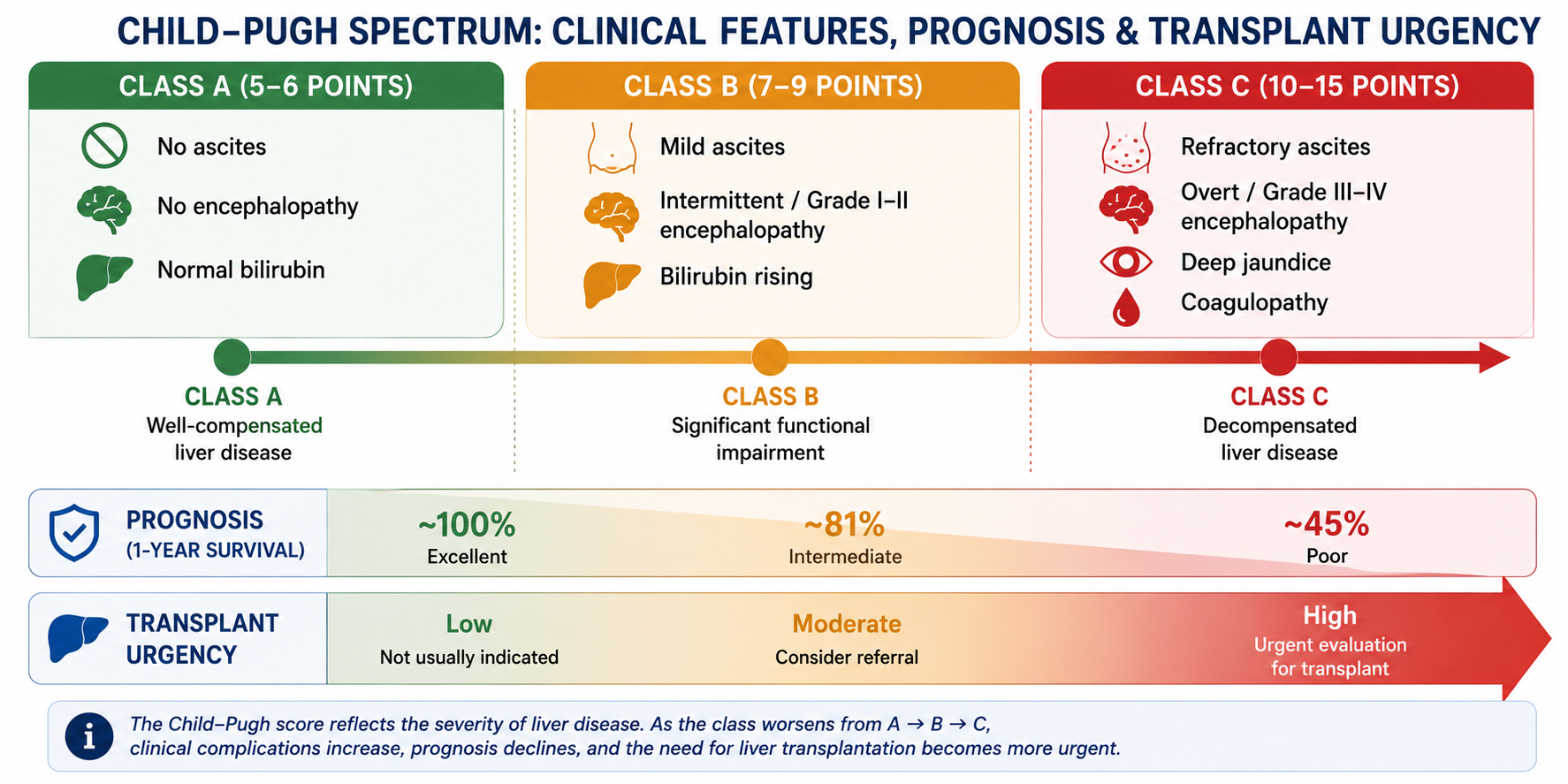
Class A — Compensated cirrhosis
Class B — Beginning decompensation
Class C — Critical / advanced decompensated disease
The survival figures above are historical averages from the original validation studies. Actual survival depends heavily on the aetiology of cirrhosis, access to specialist care, treatment of complications, and availability of liver transplantation. In modern hepatological practice, the Child-Pugh class is one prognostic input among many — it should not be used in isolation to determine prognosis in an individual patient.
Clinical Interpretation
Child-Pugh Class A
Patients in Class A have compensated cirrhosis — the liver is significantly damaged but retains enough function to maintain most homeostatic processes. These patients may have normal or near-normal bilirubin and albumin, an INR below 1.7, no ascites, and no encephalopathy. They are generally safe for elective surgery and most procedural interventions. Mortality from major surgery is estimated at around 5–10%.
Child-Pugh Class B
Class B represents significant functional compromise. Some biochemical parameters are abnormal, and complications such as mild ascites or intermittent encephalopathy may be present. Elective surgery carries substantially higher risk (estimated operative mortality 20–30% for major surgery), and close peri-operative hepatological management is required. Liver transplant evaluation should be considered.
Child-Pugh Class C
Class C indicates decompensated cirrhosis with multiple complications and very limited hepatic reserve. Operative mortality for major surgery approaches 80% or higher. Most standard surgical and oncological treatments are contraindicated. Palliative management and liver transplant listing (if eligible) are priorities.
Clinical judgement should always accompany Child-Pugh classification. Two patients with the same Child-Pugh score may have substantially different prognoses depending on age, underlying aetiology of liver disease, renal function, portal hypertension complications, and access to specialist care. The score provides a framework — it does not replace individualised clinical assessment.
Limitations of the Child-Pugh Score
Ascites and hepatic encephalopathy are scored subjectively — different clinicians may grade the same patient's ascites or HE differently. "Mild" versus "moderate" ascites and Grade I versus Grade II encephalopathy can be difficult to distinguish, introducing inter-observer variability into the score.
Renal dysfunction — particularly hepatorenal syndrome — is one of the most important prognostic determinants in decompensated cirrhosis. The Child-Pugh score does not include serum creatinine or any measure of renal function. This is a significant gap that the MELD score (which includes creatinine) partially addresses.
The maximum score is 15 (Class C). Patients with scores of 10 and 15 are both in Class C, but have very different prognoses — a score of 15 represents far more severe disease. This ceiling effect means the score loses discriminative power at the severely ill end of the spectrum.
Albumin is an acute phase reactant — it falls in acute illness, sepsis, and malnutrition independently of hepatic synthetic function. Similarly, INR can be raised by warfarin or vitamin K deficiency without reflecting true hepatic dysfunction. These confounders can inflate the Child-Pugh score inappropriately.
The Child-Pugh score was developed and validated in patients with cirrhosis and portal hypertension. It performs poorly in acute liver failure, non-cirrhotic portal hypertension, and other non-cirrhotic liver conditions.
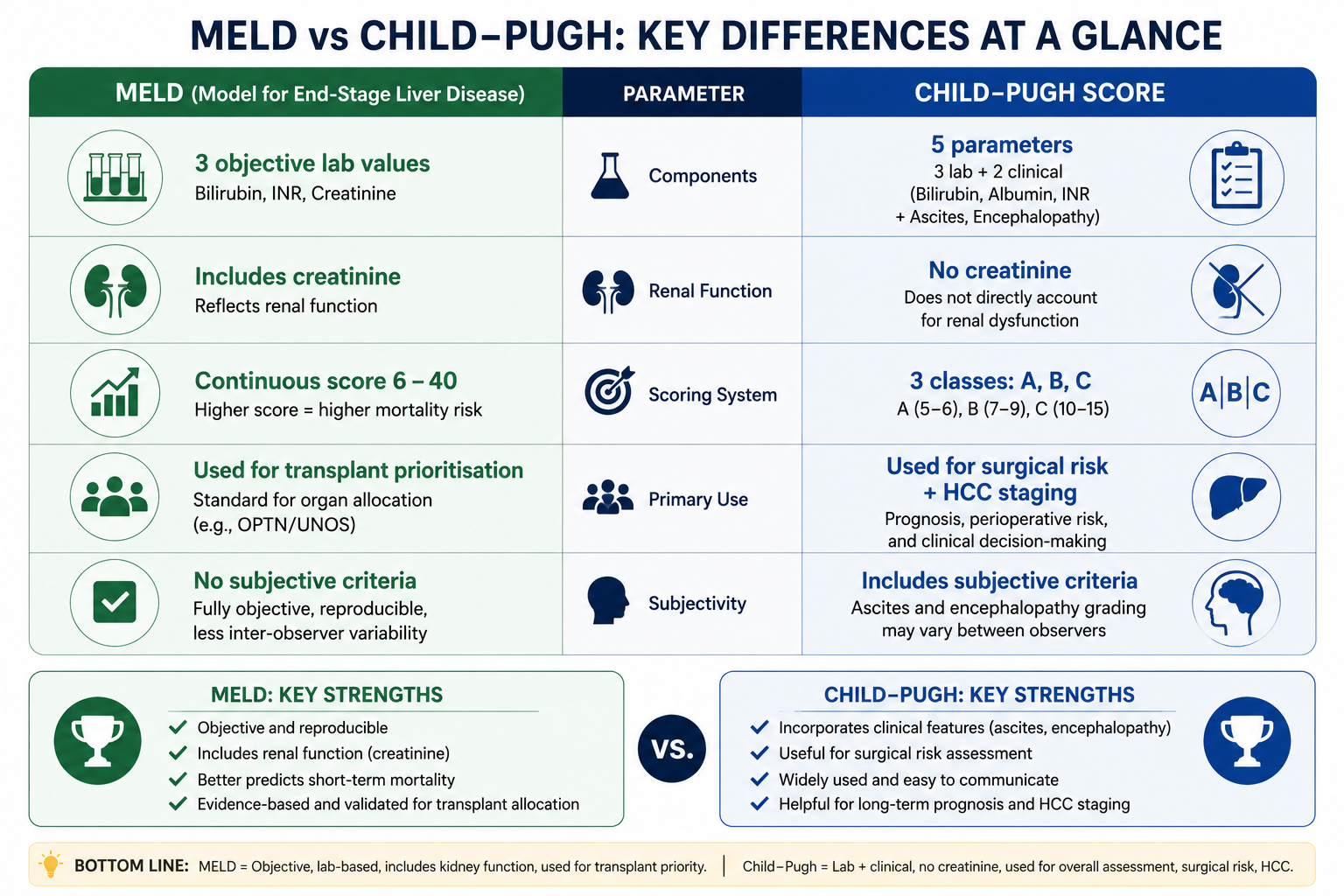
Child-Pugh remains widely used for:
- Clinical communication and disease classification
- Surgical risk assessment
- HCC staging (BCLC system)
- General severity classification in clinical practice
MELD is preferred for:
- Liver transplant prioritisation
- Objective mortality prediction
- Assessment of advanced cirrhosis with renal involvement
- Incorporation of renal dysfunction (creatinine)
Both scores remain clinically important and should be viewed as complementary rather than competing systems. See MELD Score Explained for the full MELD comparison.
Exam Tips
- Five components: Bilirubin, Albumin, INR (or PT prolongation), Ascites, Encephalopathy. Mnemonic: BAIAE.
- Each scored 1–3; total score 5–15. Class A = 5–6, B = 7–9, C = 10–15.
- INR is used, not raw PT in seconds — because INR is standardised (see INR formula).
- Albumin reflects chronic function (half-life ~20 days); INR reflects acute function (Factor VII half-life ~4–6 hours).
- Child-Pugh does not include creatinine — MELD does. MELD is preferred for transplant prioritisation.
- Ascites and encephalopathy are subjective — this is a key limitation examers ask about.
- Operative mortality: Class A ~5%, Class B ~20–30%, Class C ~80%+.
- Decompensated cirrhosis = Child-Pugh B or C with active complications (ascites, encephalopathy, variceal bleeding, jaundice).
Frequently Asked Questions
Key Takeaways
- Child-Pugh score = 5 parameters (Bilirubin, Albumin, INR, Ascites, Encephalopathy), each scored 1–3, total 5–15
- Class A (5–6): well-compensated; Class B (7–9): significant impairment; Class C (10–15): decompensated
- INR (not PT seconds) is used — it directly reflects hepatic synthetic function
- Albumin (chronic synthetic function, half-life ~20 days) and INR (acute synthetic function, Factor VII half-life ~4–6 hours) are complementary markers
- Key limitations: subjective parameters (ascites, HE), no creatinine, ceiling effect at Class C
- MELD is preferred for transplant prioritisation; Child-Pugh remains valuable for clinical staging and surgical risk assessment
- Decompensated cirrhosis = Class B or C with active complications — prognosis deteriorates sharply at decompensation
References
- Child CG, Turcotte JG. Surgery and portal hypertension. In: Child CG, ed. The Liver and Portal Hypertension. Philadelphia: Saunders; 1964:50–64.
- Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R. Transection of the oesophagus for bleeding oesophageal varices. Br J Surg. 1973;60(8):646–649.
- Durand F, Valla D. Assessment of the prognosis of cirrhosis: Child-Pugh versus MELD. J Hepatol. 2005;42(Suppl 1):S100–S107.
- D'Amico G, Garcia-Tsao G, Pagliaro L. Natural history and prognostic indicators of survival in cirrhosis: a systematic review of 118 studies. J Hepatol. 2006;44(1):217–231.
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460.
- Forner A, Reig M, Bruix J. Hepatocellular carcinoma. Lancet. 2018;391(10127):1301–1314.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and specialist hepatological input when assessing and managing patients with liver disease.