Prothrombin time (PT) and the international normalised ratio (INR) are among the most commonly ordered coagulation tests in clinical medicine. They appear in liver function assessments, anticoagulation monitoring, pre-operative panels, and critical care — yet they are frequently misunderstood.
Understanding what PT and INR actually measure, why INR replaced raw PT for inter-laboratory communication, and what causes these values to become abnormal is fundamental for any clinician interpreting blood results.
PT is the raw clotting time, measured in seconds, after tissue factor is added to plasma. INR is the standardised version of PT that allows results from different laboratories to be compared reliably.
Learning Objectives
- Explain what PT measures and which coagulation pathway it tests
- List the coagulation factors assessed by PT
- Explain the INR formula and why INR was introduced
- Describe the common causes of a prolonged PT/INR
- Distinguish clinical uses of PT versus INR
- Identify common errors in interpreting PT and INR results
What is Prothrombin Time?
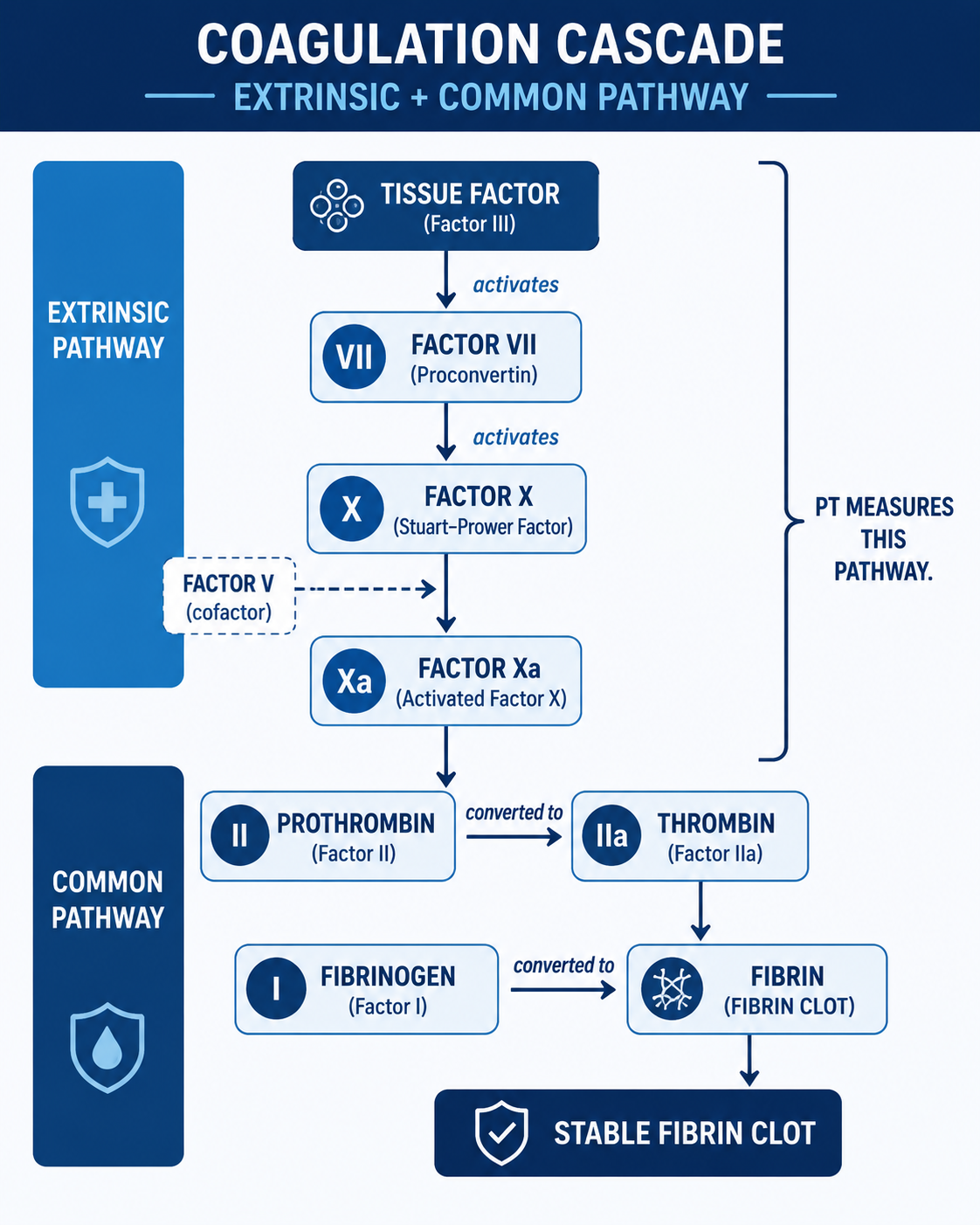
Prothrombin time is a laboratory test that measures how long (in seconds) it takes for a plasma sample to clot when tissue factor (thromboplastin) and calcium are added. Adding tissue factor activates the extrinsic pathway, which then converges into the common pathway to produce a fibrin clot.
Normal PT Range
Normal PT is approximately 11–14 seconds, though the exact reference range varies between laboratories depending on the thromboplastin reagent used. A prolonged PT indicates a deficiency or dysfunction in one or more of the relevant coagulation factors — this inter-laboratory variability is exactly why INR was developed.
Coagulation Factors Assessed by PT
PT is sensitive to deficiencies in the following coagulation factors:
| Factor | Name | Pathway | Vitamin K Dependent? | Synthesised by Liver? |
|---|---|---|---|---|
| I | Fibrinogen | Common | No | Yes |
| II | Prothrombin | Common | Yes | Yes |
| V | Factor V (labile factor) | Common | No | Yes |
| VII | Factor VII (stable factor) | Extrinsic | Yes | Yes |
| X | Factor X (Stuart factor) | Common | Yes | Yes |
Factor V is produced by the liver but is not vitamin K dependent. This matters clinically: in liver disease, all PT-relevant factors (I, II, V, VII, X) are reduced. In vitamin K deficiency or warfarin effect, only the vitamin K-dependent factors (II, VII, X) are affected — Factor V is preserved. A low Factor V with a raised INR therefore points to liver disease rather than vitamin K deficiency.
The remaining coagulation factors (VIII, IX, XI, XII) are assessed by the activated partial thromboplastin time (APTT), which tests the intrinsic and common pathways. PT and APTT are complementary investigations.
What is INR?
The international normalised ratio (INR) is a standardised expression of the prothrombin time, corrected for inter-laboratory variation. It is calculated as:
INR does not measure a separate biological process. It is a mathematically standardised expression of the PT. The underlying laboratory reaction is still the PT test; INR simply corrects that PT result so it can be compared across laboratories.
INR is a dimensionless ratio — it has no units. In a healthy, non-anticoagulated adult the INR is approximately 0.8–1.2. For a step-by-step breakdown of the calculation, see How INR Is Calculated.
Why INR Was Developed
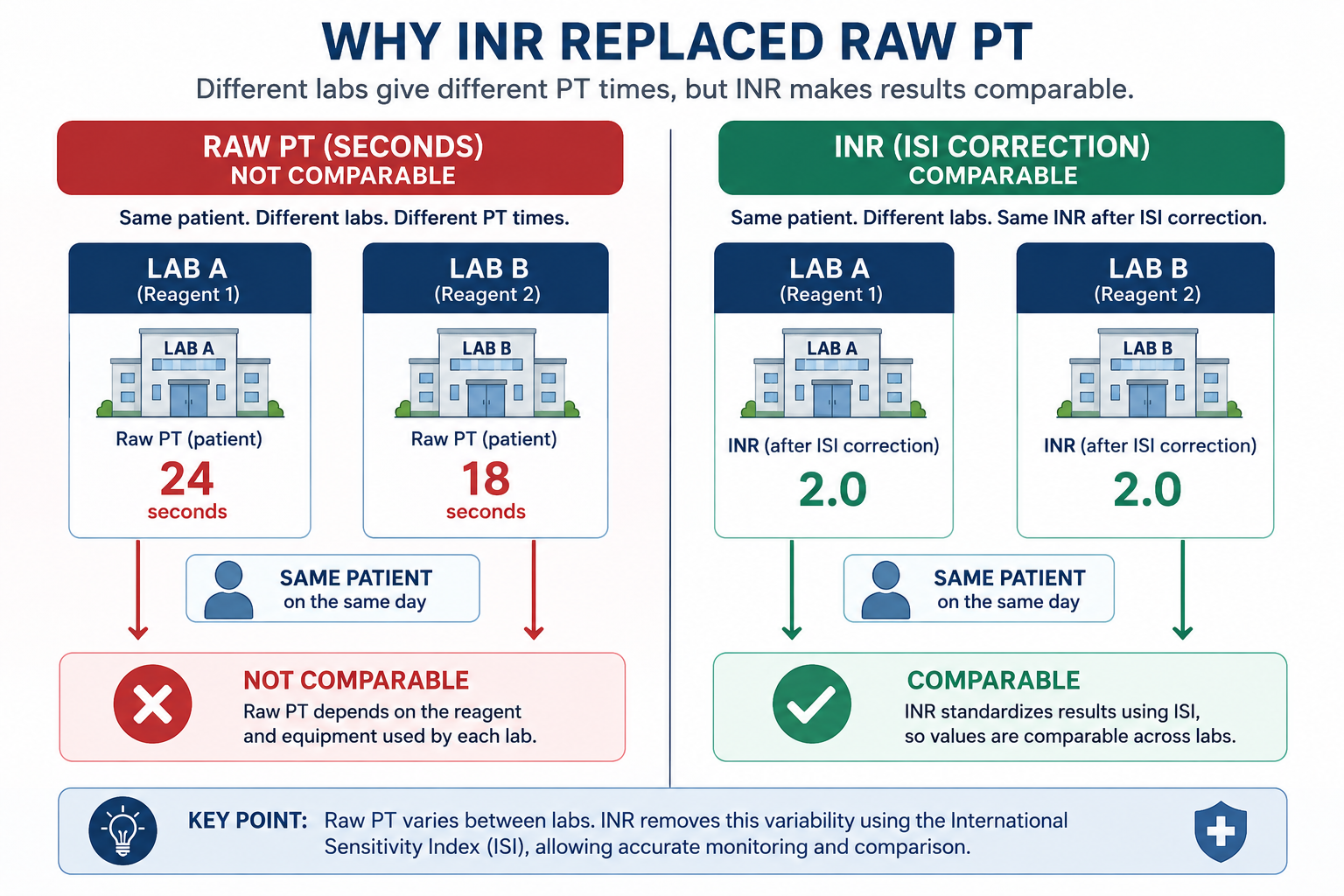
Before INR, clinicians monitored warfarin using raw PT in seconds. The problem: different laboratories used different thromboplastin reagents to perform the test. Because reagents varied in their sensitivity to clotting factor deficiencies, the same patient's blood could produce a PT of 20 seconds at one hospital and 27 seconds at another — making inter-laboratory comparison impossible and warfarin dosing decisions unreliable.
Before INR standardisation, the same patient could have a PT of 18 seconds in one laboratory and 24 seconds in another because different thromboplastin reagents had different sensitivities. This made warfarin monitoring and inter-hospital communication unreliable. INR was introduced specifically to solve this problem.
The World Health Organization introduced the INR system in the 1980s. By calibrating each laboratory's thromboplastin against a WHO reference preparation and assigning it an ISI value, the INR formula converts any lab's raw PT into a standardised ratio that means the same thing everywhere. For a full explanation of ISI, see ISI Explained.
Always use INR — not raw PT in seconds — when communicating coagulation status across institutions, monitoring warfarin, or documenting liver synthetic function in scoring systems.
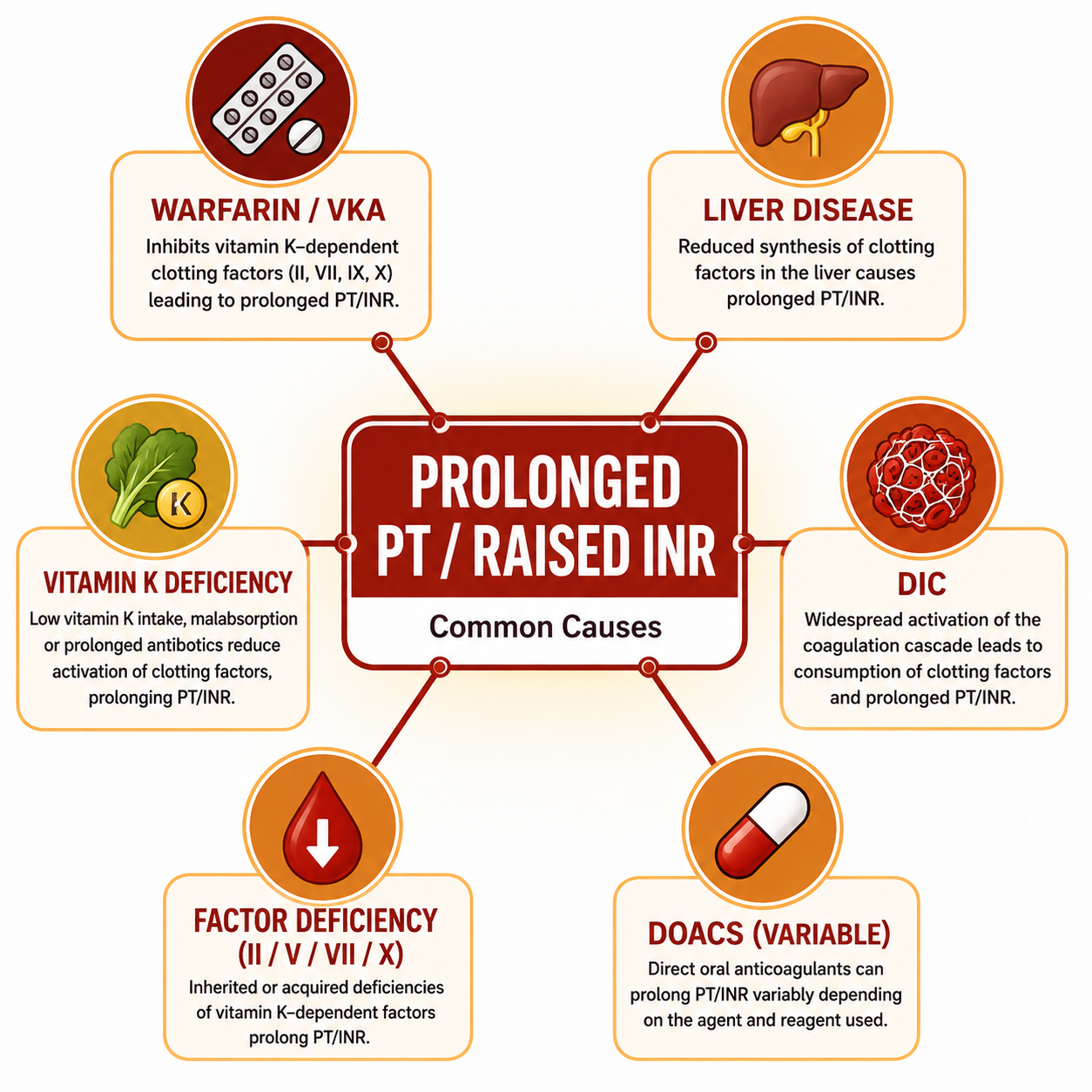
Common Causes of Prolonged PT/INR
1. Warfarin (Vitamin K Antagonist)
Warfarin inhibits the vitamin K epoxide reductase enzyme, reducing the hepatic synthesis of vitamin K-dependent clotting factors (II, VII, IX, X). Because Factors II, VII, and X are assessed by PT, warfarin prolongs PT and raises INR. This is the basis of warfarin monitoring. Therapeutic INR targets vary by indication (see Clinical Uses section).
2. Liver Disease
The liver synthesises all five factors tested by PT (I, II, V, VII, X). In significant hepatic dysfunction (cirrhosis, acute liver failure), synthesis of these factors is impaired, prolonging PT and raising INR. INR directly reflects hepatic synthetic function and is a component of both the Child-Pugh score and the MELD score.
3. Vitamin K Deficiency
Vitamin K is a fat-soluble vitamin required for the carboxylation and activation of Factors II, VII, IX, and X. Deficiency arises from malnutrition, fat malabsorption (cholestatic liver disease, coeliac disease, pancreatic insufficiency), prolonged broad-spectrum antibiotics, or in neonates (haemorrhagic disease of the newborn). Unlike in liver disease, Factor V levels are preserved.
4. Disseminated Intravascular Coagulation (DIC)
Widespread coagulation cascade activation in DIC causes consumption of clotting factors and platelets. Both PT and APTT are typically prolonged; fibrinogen falls and D-dimers rise. DIC is a clinical emergency requiring urgent management of the underlying trigger.
5. Factor Deficiencies
Inherited or acquired deficiency of Factor I, II, V, VII, or X prolongs PT. Isolated Factor VII deficiency prolongs PT without affecting APTT, since Factor VII is the only factor exclusive to the extrinsic pathway. Combined factor deficiencies or severe hypofibrinogenaemia also prolong PT.
6. Direct Oral Anticoagulants (DOACs)
Factor Xa inhibitors (rivaroxaban, apixaban, edoxaban) and the direct thrombin inhibitor dabigatran can prolong PT to varying and unpredictable degrees. PT is not validated for monitoring DOAC therapy — specific anti-Xa or anti-thrombin assays are required.
PT vs INR: Comparison
| Feature | PT (seconds) | INR |
|---|---|---|
| What it measures | Raw clotting time via extrinsic + common pathway | Standardised ratio derived from PT |
| Units | Seconds | Dimensionless ratio |
| Normal range | ~11–14 s (lab-dependent) | 0.8–1.2 |
| Comparable between labs? | No — varies with reagent | Yes — standardised via ISI |
| Used for warfarin monitoring? | Not recommended | Yes — gold standard |
| Used in liver scoring? | Rarely used alone | Yes (Child-Pugh, MELD) |
PT = laboratory measurement.
INR = standardised expression of that measurement.
Raw PT values are laboratory-dependent; INR is designed for comparison across laboratories.
Clinical Uses of PT and INR
1. Warfarin Monitoring
INR is the gold standard for monitoring oral anticoagulation with warfarin. Therapeutic targets vary by indication:
| Indication | Target INR |
|---|---|
| Atrial fibrillation (stroke prevention) | 2.0–3.0 |
| DVT / PE treatment | 2.0–3.0 |
| Mechanical mitral valve | 2.5–3.5 |
| Mechanical aortic valve (low risk) | 2.0–3.0 |
| Recurrent thromboembolism on anticoagulation | 3.0–4.0 |
2. Liver Synthetic Function
In liver disease, a rising INR reflects worsening hepatic synthetic capacity. It is a key component of the Child-Pugh classification and the MELD score, used to stratify severity of chronic liver disease and guide transplant listing decisions. For more detail, read Child-Pugh Score Explained and MELD Score Explained.
3. Pre-Operative Assessment
INR is checked pre-operatively in patients on anticoagulants, those with known or suspected bleeding disorders, or those with liver disease. Most elective procedures can be safely performed with INR ≤ 1.5. Higher values require correction with vitamin K, fresh frozen plasma (FFP), or prothrombin complex concentrate (PCC) depending on urgency.
4. Localising Coagulopathies
Used alongside APTT, PT helps localise a coagulopathy: isolated prolonged PT suggests the extrinsic pathway (Factor VII deficiency, early warfarin effect); isolated prolonged APTT suggests the intrinsic pathway (Factors VIII, IX, XI, XII); both prolonged suggests the common pathway or a global coagulopathy (DIC, severe liver disease).
Common Mistakes
PT (seconds) and INR are not the same. PT is the raw clotting time; INR applies the ISI correction. They only coincide numerically when ISI = 1.0, which is rare in practice. Never use raw PT seconds interchangeably with INR across different hospitals.
PT/INR does not assess platelet function, von Willebrand factor, or the intrinsic pathway (Factors VIII, IX, XI). A patient with severe thrombocytopaenia or haemophilia A can have a completely normal INR yet be at high risk of clinically significant bleeding.
DOACs variably affect PT but the change does not reliably reflect anticoagulant effect. Specific assays are required for DOAC quantification. Never use PT/INR to determine DOAC adequacy or safety for surgery.
In compensated cirrhosis, both pro- and anticoagulant factor production is reduced, often preserving haemostatic balance despite a raised INR. Routine FFP infusion to "correct" INR pre-procedure is not routinely justified and may cause harm. Always seek specialist input before correcting coagulopathy in liver disease.
Exam Tips
- PT tests extrinsic + common pathway (Factors I, II, V, VII, X); APTT tests intrinsic + common pathway.
- Factor VII has the shortest half-life (~4–6 hours) — PT is the first coagulation test to become abnormal in acute liver failure or on starting warfarin.
- Prolonged PT, normal APTT → warfarin, early liver disease, Factor VII deficiency, early vitamin K deficiency.
- Both PT and APTT prolonged → severe liver disease, DIC, massive transfusion, supratherapeutic anticoagulation, common pathway deficiency.
- INR is used in both MELD and Child-Pugh scoring — know both scoring systems and what they predict.
- Warfarin takes 3–5 days for full effect because it waits for existing vitamin K-dependent factors to be depleted, especially Factor II (half-life ~60 hours).
- Factor V low + raised INR → liver disease; Factor V normal + raised INR → vitamin K deficiency or warfarin.
- INR does not assess platelet number or platelet function — a normal INR does not exclude thrombocytopaenia, platelet dysfunction, or von Willebrand disease.
Frequently Asked Questions
Key Takeaways
- PT measures clotting time via the extrinsic + common pathway and tests Factors I, II, V, VII, and X
- INR is PT standardised using the ISI correction — it is comparable between laboratories; raw PT in seconds is not
- Normal INR (non-anticoagulated adult): 0.8–1.2
- Raised INR: warfarin, liver disease, vitamin K deficiency, DIC, factor deficiencies
- Factor VII has the shortest half-life — PT/INR is the first coagulation test to become abnormal in acute liver failure
- Factor V preserved + raised INR → vitamin K deficiency/warfarin; Factor V low + raised INR → liver disease
- INR is a component of the Child-Pugh score and the MELD score
- Normal INR does not exclude platelet disorders, von Willebrand disease, or intrinsic pathway deficiencies
References
- WHO Expert Committee on Biological Standardization. Guidelines for thromboplastins and plasma used to control oral anticoagulant therapy. WHO Technical Report Series No. 889. Geneva: WHO; 1999.
- Tripodi A, Mannucci PM. The coagulopathy of chronic liver disease. N Engl J Med. 2011;365(2):147–156.
- Keeling D, et al. Guidelines on oral anticoagulation with warfarin (4th ed.). Br J Haematol. 2011;154(3):311–324.
- Hunt BJ. Bleeding and coagulopathies in critical care. N Engl J Med. 2014;370(9):847–859.
- Lippi G, Favaloro EJ. Laboratory hemostasis: from biology to the bench. Clin Chem Lab Med. 2018;56(7):1118–1130.
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines and senior clinical input when interpreting coagulation results and managing patients.