CT is the first-line imaging investigation in acute head trauma. It is rapid, widely available, and highly sensitive for detecting immediately life-threatening intracranial injuries.
For medical students, intern doctors, and junior doctors working in emergency and acute settings, the ability to recognise major CT findings in traumatic brain injury (TBI) is a core clinical skill. Prompt identification of critical findings — such as an expanding epidural haematoma, uncal herniation, or diffuse cerebral swelling — directly influences patient outcomes.
This article provides a systematic approach to reviewing a trauma head CT, followed by detailed descriptions of the most common and clinically important findings. Each section covers the imaging features, clinical context, and exam-relevant points.
Learning Objectives
- Describe the principles of CT density and apply Hounsfield units to interpreting head CT
- Follow a systematic approach to reviewing a trauma head CT
- Identify the imaging features of epidural haematoma (EDH) and subdural haematoma (SDH)
- Distinguish traumatic subarachnoid haemorrhage from spontaneous SAH
- Describe the appearance of intracerebral haemorrhage and cerebral contusions
- Identify skull fractures on CT bone windows
- Recognise signs of mass effect, midline shift, and cerebral herniation
- Identify post-traumatic hydrocephalus, pneumocephalus, and cerebral oedema
- Recognise diffuse axonal injury (DAI) on CT and explain why MRI is more sensitive
- Apply appropriate CT window settings to identify different categories of pathology
- Structure and present trauma CT findings in a systematic, clinically useful way
CT Density Basics
CT images are produced by measuring X-ray beam attenuation through tissues. The resulting values are expressed in Hounsfield units (HU). By convention, water = 0 HU and air = −1000 HU. Dense materials (e.g. bone) absorb more X-rays and appear white; less dense materials (e.g. air) appear black.
In head CT, structures are described relative to adjacent brain parenchyma:
- Hyperdense (bright/white) — higher attenuation than brain, e.g. acute blood, calcification, bone
- Isodense — similar attenuation to brain, e.g. subacute blood (days 3–21)
- Hypodense (dark/black) — lower attenuation than brain, e.g. oedema, CSF, old blood, air
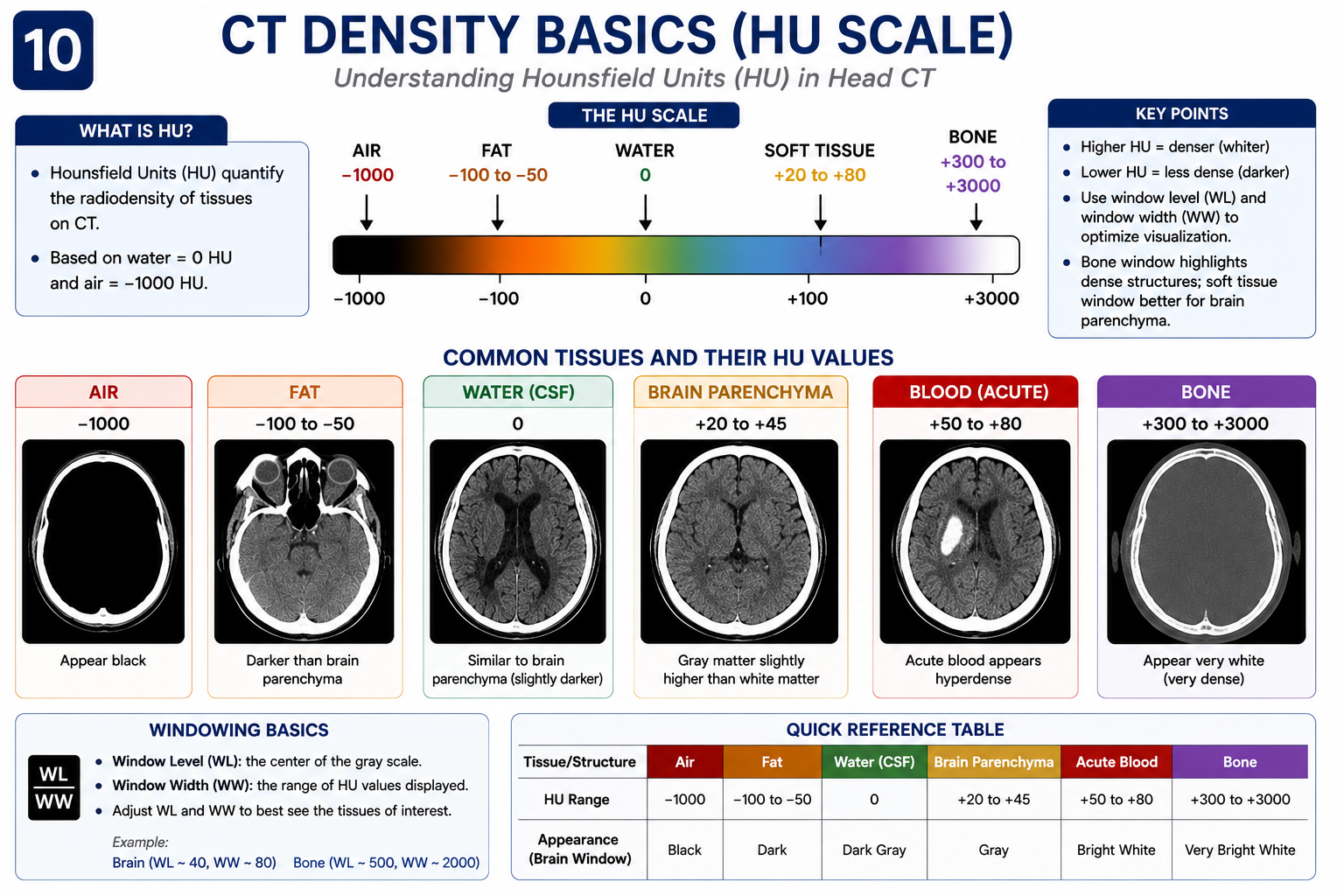
| Structure / Finding | Approx. HU | CT Appearance |
|---|---|---|
| Cortical bone | 400–1000 | Hyperdense (white) |
| Acute haemorrhage | 60–90 | Hyperdense (white) |
| Grey matter | 35–40 | Isodense |
| White matter | 20–30 | Isodense |
| Subacute blood (~day 3–21) | ~35–40 | Isodense |
| CSF / water | ~0 | Hypodense (dark) |
| Cerebral oedema | 10–25 | Hypodense (dark) |
| Chronic blood (>3 weeks) | <20 | Hypodense (dark) |
| Air | ~−1000 | Black |
Acute blood is hyperdense due to the high protein content of clotted haemoglobin. As blood breaks down over days to weeks, it becomes progressively isodense and then hypodense. Understanding this density evolution is essential for dating subdural haematomas and recognising isodense collections that are easily missed.
Understanding CT Window Settings
The same CT scan can be viewed using different window settings. Each window adjusts the brightness and contrast of the displayed image to optimise visualisation of a specific tissue type. Choosing the correct window is essential — some findings are difficult or impossible to identify on inappropriate settings.
| Window | Width / Level (approx.) | Main Use |
|---|---|---|
| Brain (soft tissue) | W 80 / L 40 | Intracranial haemorrhage, oedema, parenchymal injury, grey–white differentiation |
| Bone | W 3000 / L 600 | Skull fractures, facial fractures, skull base injuries — always review in trauma |
| Subdural | W 150–200 / L 50–75 | Subtle subdural collections and extra-axial blood; makes isodense SDH more visible |
| Soft tissue | W 350 / L 60 | Scalp swelling and extracranial soft tissue injuries |
Many skull fractures are invisible on standard brain windows and become obvious only when the bone window is reviewed. Never report a trauma CT as normal without having reviewed the bone window. Similarly, a narrow subdural window can reveal subtle extra-axial collections that appear isodense and are easily missed on routine brain windows.
A Systematic Approach to Trauma Head CT
Systematic review of a trauma head CT reduces the risk of missing significant findings. The mnemonic BATTERS provides a reliable framework:
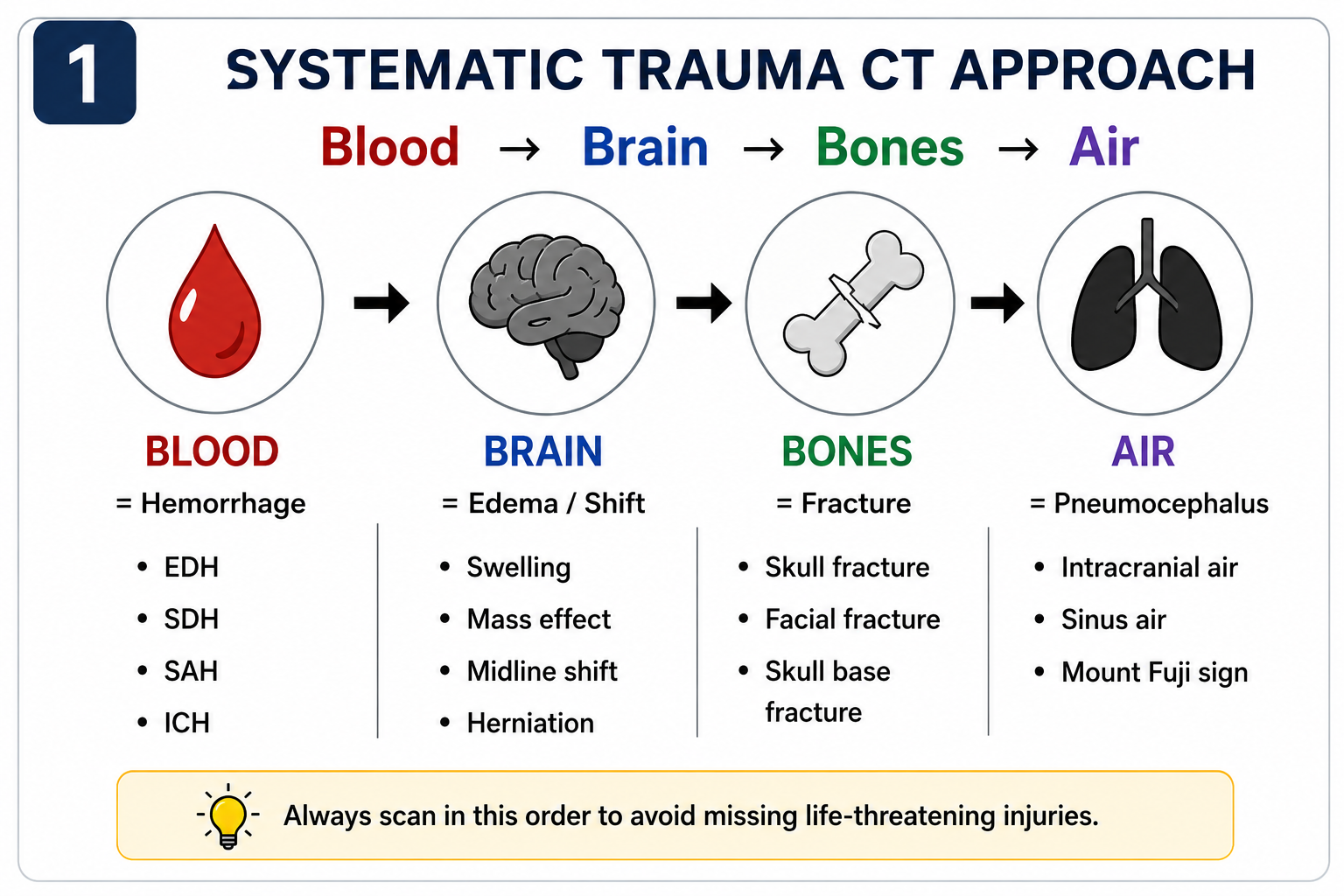
| Letter | Stands For | What to Assess |
|---|---|---|
| B | Blood | Extra-axial (EDH, SDH, SAH) and intra-axial (ICH, contusions) haemorrhage |
| A | Asymmetry / Arteries | Asymmetry of sulci, gyri, and ventricles; vascular injury on CT angiography if indicated |
| T | Tissue (parenchyma) | Focal oedema, contusions, grey–white differentiation, diffuse axonal injury |
| T | Trauma (bone) | Skull fractures on bone windows — linear, depressed, basilar, diastatic |
| E | Extra-axial spaces | Review all compartments including tentorium, falx, and posterior fossa |
| R | Raised ICP signs | Midline shift, sulcal effacement, cisternal compression, herniation |
| S | Subarachnoid / Skull base | SAH in sulci and cisterns; skull base fractures |
Always view the CT on multiple window settings. The standard brain window is best for parenchyma and haemorrhage. Use the bone window to assess skull fractures. A subdural window (narrowed width) makes subtle subdural collections more visible.
Normal CT Brain Anatomy
Recognising the normal CT brain is essential before identifying pathology. A normal CT shows symmetrical grey and white matter with clear grey–white differentiation, midline structures in the midline, open symmetrical sulci and cisterns, and normal-sized ventricles with CSF-density contents.
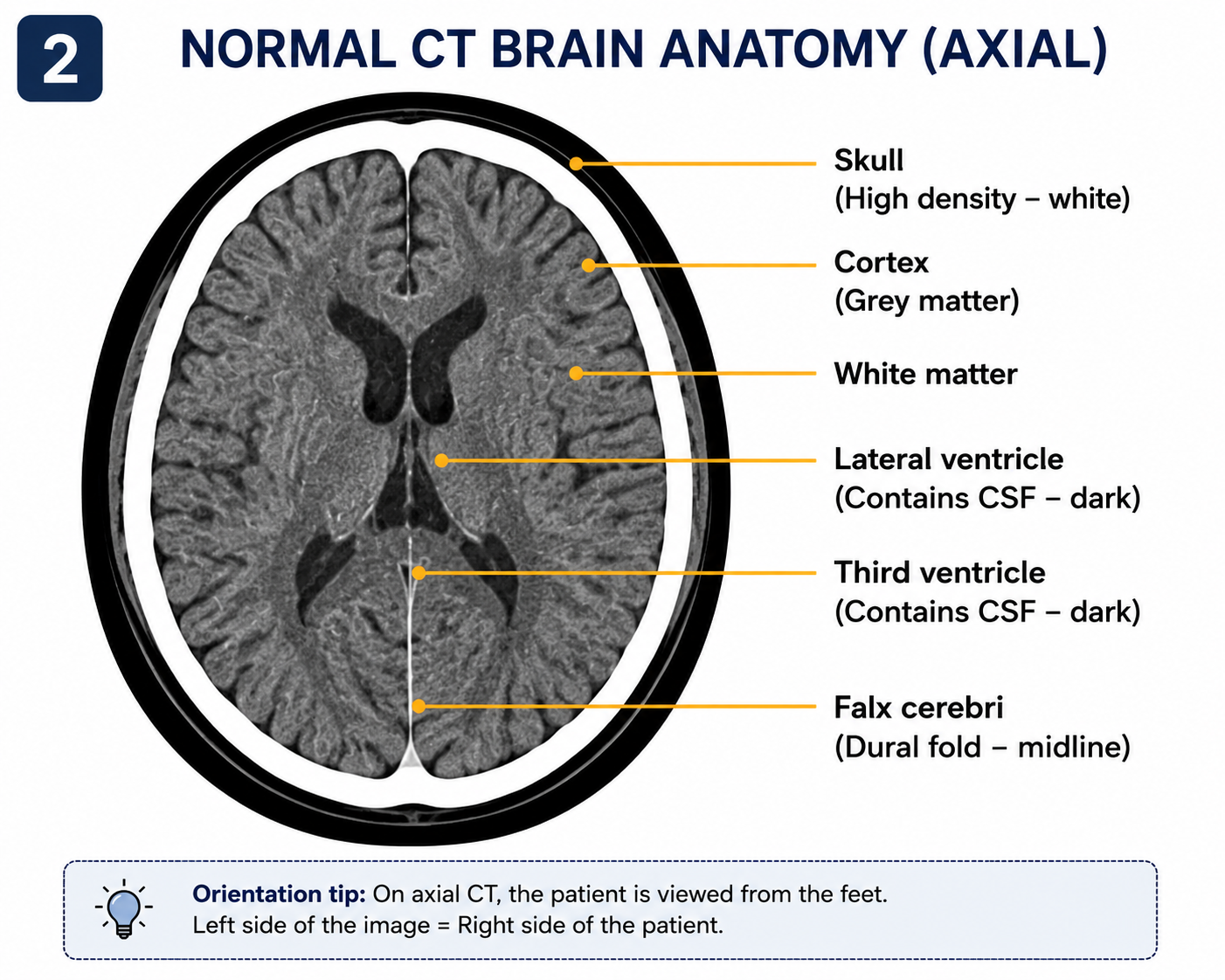
- Basal cisterns — obliteration or asymmetry indicates raised ICP or transtentorial herniation
- Sylvian fissures — blood here suggests traumatic SAH or SDH
- Interhemispheric fissure — linear hyperdensity may indicate SAH or subfrontal haematoma
- Temporal horns — dilation may indicate acute obstructive hydrocephalus
- Septum pellucidum — displacement from midline indicates mass effect
Epidural Haematoma (EDH)
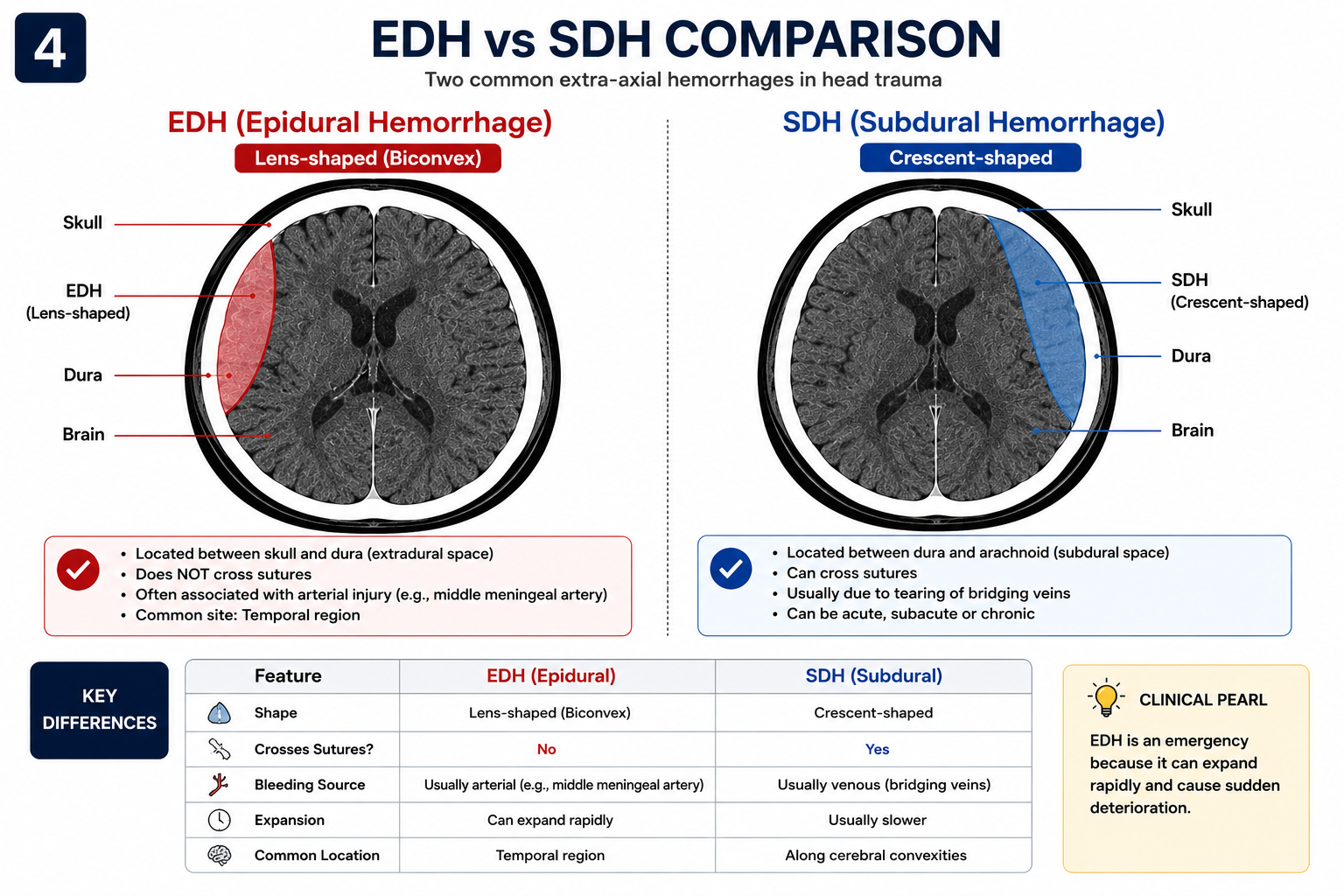
An epidural haematoma (EDH) is a collection of blood between the inner skull surface and the outer layer of the dura. It most commonly results from rupture of the middle meningeal artery following a temporal bone fracture through the pterion — the thinnest and weakest part of the skull.
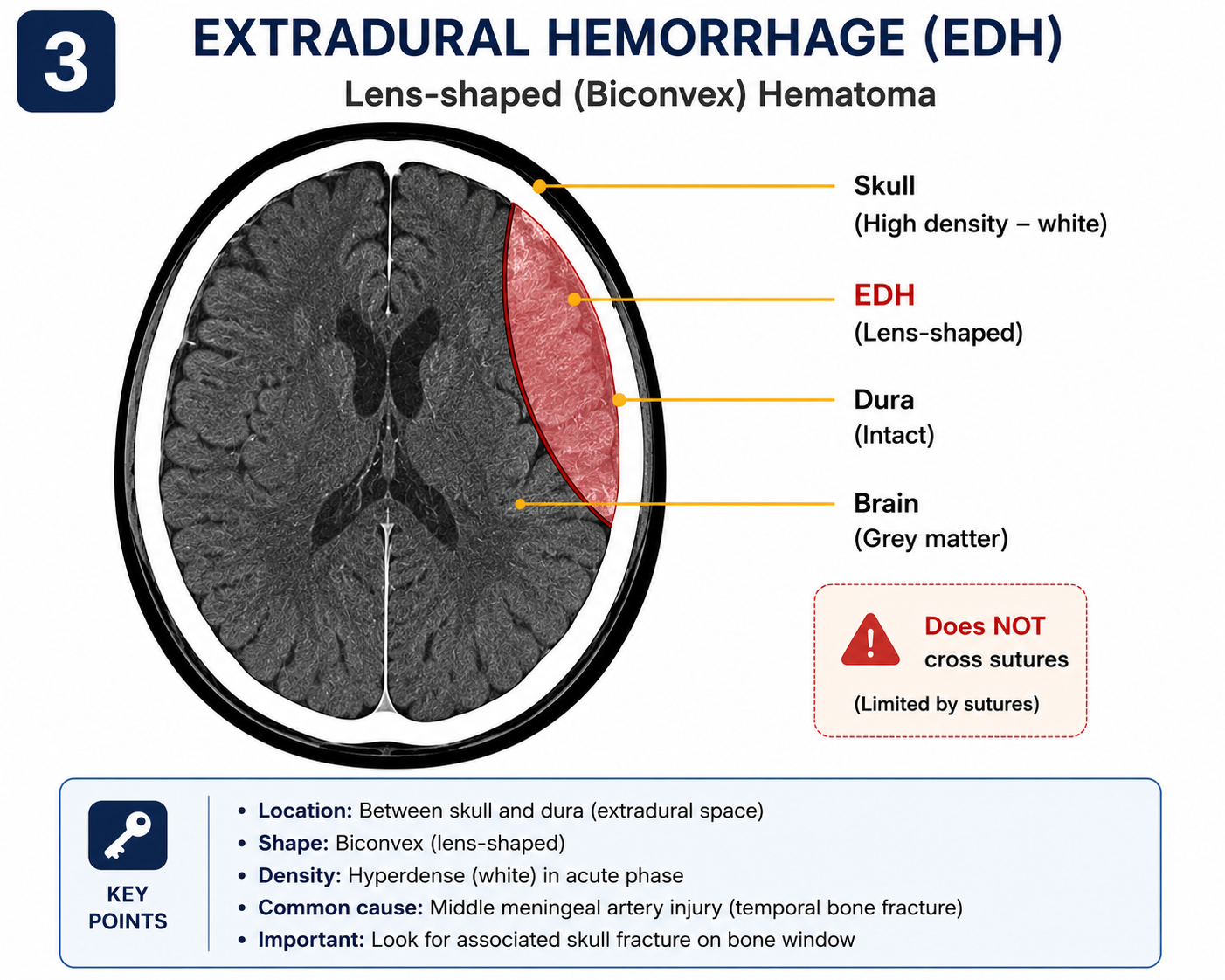
CT Appearance
- Shape: Biconvex (lenticular / lens-shaped) — the dura strips from the inner skull surface but remains tethered at suture lines, creating a convex medial border
- Density: Hyperdense in acute phase (60–90 HU)
- Location: Temporal most common (pterion); also frontal, parietal, or posterior fossa
- Suture lines: Does not cross suture lines — a key distinguishing feature from SDH
- Swirl sign: Mixed hyperdense and hypodense swirling areas within the collection, indicating active ongoing arterial bleeding — a critical finding requiring immediate surgical intervention
Clinical Features
The classic presentation is the lucid interval: brief loss of consciousness at impact, then apparent recovery, followed by rapid neurological deterioration as the haematoma expands. In practice, only a minority of patients demonstrate this classic triad — do not exclude EDH because a lucid interval is absent.
EDH is a time-critical surgical emergency. Urgent craniotomy is indicated for haematoma volume >30 mL, thickness >15 mm, or midline shift >5 mm. Even smaller collections require close monitoring, as rapid expansion — especially if the swirl sign is present — can occur within minutes.
EDH is more common in younger patients because the dura is less firmly adherent to the skull, allowing blood to strip the dura more easily. In the elderly, the dura is more tightly adherent, making EDH less common but SDH more likely after the same mechanism of injury.
Subdural Haematoma (SDH) and Comparison with EDH
A subdural haematoma (SDH) is a collection of blood in the subdural space — between the inner dural layer and the arachnoid. It typically results from tearing of bridging veins that run from the brain surface to the dural venous sinuses. SDH is more common than EDH and is frequently seen in elderly patients, those on anticoagulants, and patients with alcohol-related cerebral atrophy.
CT Appearance — Acute SDH
- Shape: Crescent-shaped, following the contour of the brain surface
- Location: Convexity most common; can also be bilateral, interhemispheric, or in posterior fossa
- Suture lines: Crosses suture lines (unlike EDH)
- Density evolution: Acute (<72 h): hyperdense → Subacute (day 3–21): isodense → Chronic (>3 weeks): hypodense
- Associated findings: Frequently accompanied by underlying brain injury, oedema, and significant mass effect
| Feature | EDH | SDH |
|---|---|---|
| Location | Between skull and dura | Between dura and arachnoid |
| Shape | Biconvex (lenticular) | Crescent-shaped |
| Crosses sutures? | No | Yes |
| Source of bleed | Arterial (middle meningeal artery) | Venous (bridging veins) |
| Common in | Young adults; skull fracture | Elderly, anticoagulated, cerebral atrophy |
| Classic presentation | Lucid interval (minority) | Variable; insidious onset possible in chronic SDH |
| Acute CT density | Hyperdense | Hyperdense; evolves to isodense then hypodense |
| Underlying brain injury | Less common | Common and often contributes to morbidity |
The isodense subdural haematoma (subacute phase, ~day 3–21) is a classic exam pitfall. Blood has become the same density as adjacent brain and can be invisible on routine windows. Look for indirect signs: sulcal effacement over one hemisphere, midline shift out of proportion to the visible collection, asymmetry of the grey–white junction, or displaced cortical veins.
Traumatic Subarachnoid Haemorrhage (SAH)
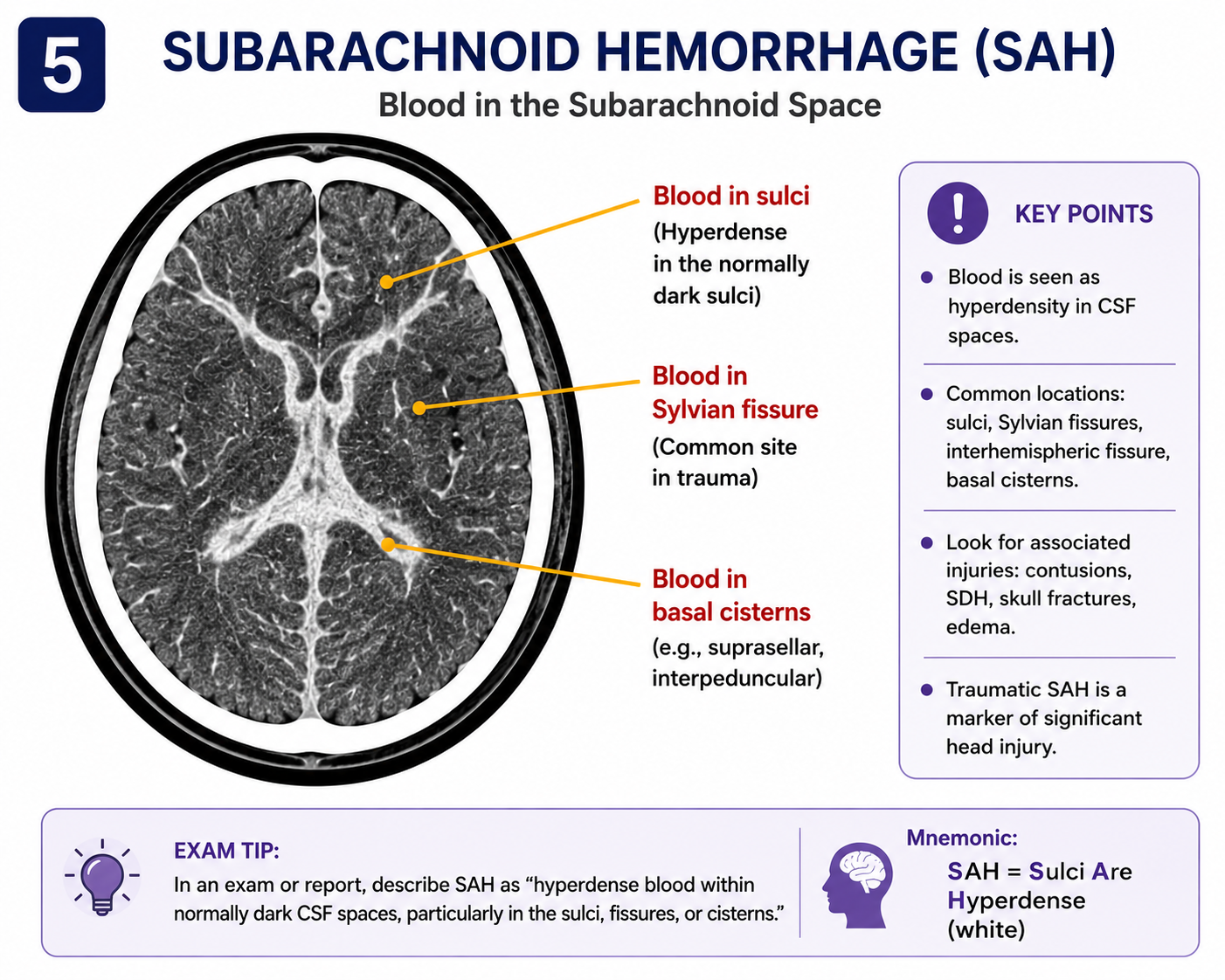
Traumatic SAH is the most common type of intracranial haemorrhage in head trauma. Blood enters the subarachnoid space through laceration of pial vessels or extension from adjacent contusions. It may also be caused by tearing of perforating arteries in the brainstem cisterns in severe injuries.
CT Appearance
- Hyperdense (white) blood within the subarachnoid space — sulci, Sylvian fissures, interhemispheric fissure, and/or basal cisterns
- Can be very subtle — requires careful inspection of every sulcus on every slice
- CT is approximately 95–99% sensitive for SAH within 6 hours; sensitivity decreases rapidly after 12–24 hours as blood dilutes
Traumatic vs Spontaneous (Aneurysmal) SAH
| Feature | Traumatic SAH | Aneurysmal SAH |
|---|---|---|
| Distribution | Convexity sulci; follows trauma mechanism | Basal cisterns; star pattern around brainstem; focal thick collection suggests aneurysm location |
| Presentation | Following trauma or fall | Thunderclap headache ("worst ever"); may lack head injury history |
| Associated findings | Skull fractures, contusions, scalp haematoma | Thick basal cistern blood; possible hydrocephalus; no bony injury |
A fall in an older patient can be the result — not the cause — of a spontaneous intracranial event. If the SAH distribution is atypical for trauma (e.g. thick basal cistern blood without skull fractures), do not assume the SAH is traumatic. Arrange urgent CT angiography or neurosurgical review to exclude an underlying aneurysm.
Complications
- Communicating hydrocephalus — blood impairs CSF reabsorption at the arachnoid granulations
- Cerebral vasospasm — most relevant in aneurysmal SAH; causes delayed ischaemia 3–14 days post-bleed
Intracerebral Haemorrhage and Cerebral Contusions
Traumatic intracerebral haemorrhage (ICH) and cerebral contusions represent intra-axial injuries — haemorrhage within the brain parenchyma itself. They frequently coexist and form part of a spectrum of severity in TBI.

Cerebral Contusions
Contusions are haemorrhagic bruises of the brain parenchyma caused by the brain striking the rough inner surface of the skull. They occur classically at the frontal and temporal poles due to the irregular bony surfaces in the anterior and middle cranial fossae.
- Coup injury: Contusion at the site of direct impact
- Contrecoup injury: Contusion on the opposite side, often larger than the coup, caused by the brain rebounding against the far skull surface
- CT appearance: Irregular, heterogeneous ("salt and pepper") areas — hyperdense haemorrhagic foci with surrounding hypodense oedema
Haemorrhagic Progression ("Blossoming")
Contusions may appear deceptively small on initial CT but can blossom (enlarge substantially) on repeat imaging 24–48 hours later. This progression is caused by ongoing microhaemorrhage, oedema expansion, and blood-brain barrier breakdown. Patients with significant contusions require serial CT imaging even if neurologically stable initially.
Haemorrhagic contusions are often associated with diffuse axonal injury (DAI), which may be invisible on initial CT. If neurological deficit is disproportionately severe relative to CT findings, suspect DAI — it is best demonstrated on MRI with gradient echo or susceptibility-weighted imaging (SWI) sequences.
Diffuse Axonal Injury (DAI)
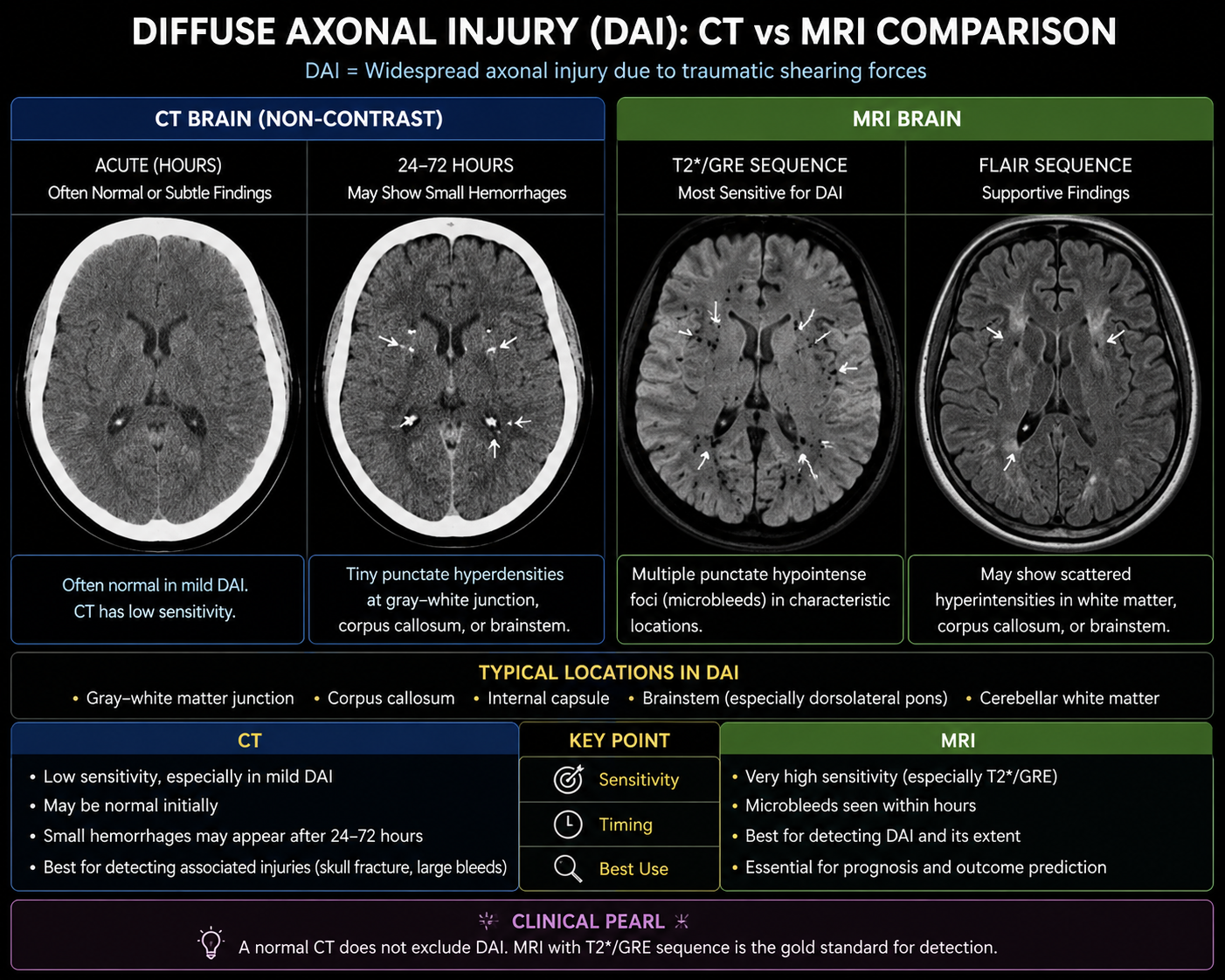
Diffuse axonal injury is a shearing injury caused by rapid acceleration-deceleration forces that stretch and tear axons throughout the brain. It commonly occurs following high-speed road traffic collisions, falls from height, and severe rotational trauma. DAI is one of the most important causes of severe neurological disability after TBI.
Unlike an epidural or subdural haematoma — discrete collections that are clearly visible on CT — DAI produces widespread microscopic axonal disruption rather than a single large collection of blood. For this reason, CT may appear largely normal or show only subtle findings despite severe neurological impairment. This is the defining clinical challenge of DAI.
Common Locations of DAI
- Grey–white matter junction (lobar white matter) — most common; seen in mild-moderate DAI
- Corpus callosum — splenium particularly; suggests moderate-severe DAI
- Brainstem (dorsolateral midbrain and pons) — indicates severe DAI; strongly associated with poor outcome
- Internal capsule and basal ganglia — less common; indicates severe injury
CT Appearance
- Small punctate haemorrhages at the grey–white junction or in the corpus callosum
- Tiny hyperdense foci in the locations above (<1 cm)
- Loss of grey–white differentiation (in severe diffuse injury)
- Diffuse cerebral swelling without a discrete haematoma
- Normal CT in mild and moderate DAI — absence of CT findings does not exclude significant axonal injury
MRI in DAI
MRI is substantially more sensitive than CT for detecting DAI. Susceptibility-weighted imaging (SWI) and gradient echo (GRE) sequences detect haemosiderin deposition from microhaemorrhages that are invisible on CT. FLAIR sequences reveal non-haemorrhagic axonal shearing. MRI is the investigation of choice when DAI is clinically suspected but CT is unremarkable.
If a patient has severe neurological impairment — coma, decerebrate posturing, or profound amnesia — but the CT appears relatively normal or shows only minor findings, diffuse axonal injury should be strongly suspected. Arrange urgent MRI brain with SWI sequences. The severity of DAI is the most important determinant of outcome in closed head injury, yet it is the finding most commonly underestimated on CT.
Skull Fractures
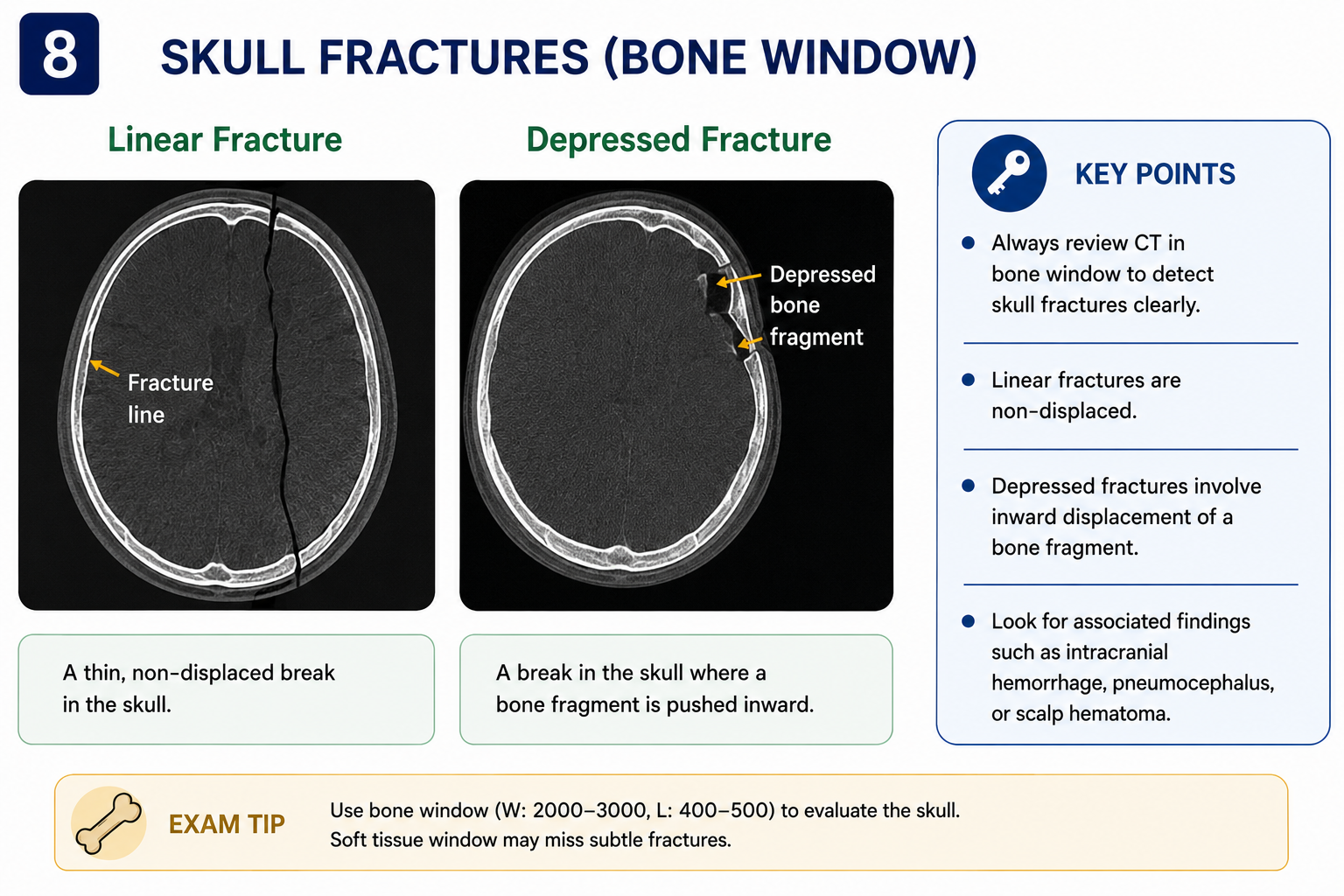
Skull fractures are identified on bone window settings. Their presence significantly increases the likelihood of an underlying intracranial haematoma, particularly EDH. Basilar fractures carry additional risk of CSF leak and meningitis.
| Type | Description | Clinical Significance |
|---|---|---|
| Linear | Simple fracture line, no bony displacement | Most common; risk of EDH if near meningeal vascular grooves or pterion |
| Depressed | Bone fragment pushed inward beyond inner table | Risk of underlying cortical laceration; may require surgical elevation |
| Comminuted | Multiple fracture fragments | Indicates high-energy impact; higher risk of associated intracranial injury |
| Diastatic | Fracture along or widening of a suture line | More common in children; may be mistaken for a normal suture |
| Basilar | Fracture of skull base — petrous temporal, sphenoid, or occipital bones | Risk of CSF leak (rhinorrhoea, otorrhoea), ascending meningitis, cranial nerve injury |
Basilar fractures may be subtle on CT but are suggested clinically by:
- Battle's sign — retroauricular (mastoid) bruising, appearing 1–3 days post-injury
- Raccoon/panda eyes — bilateral periorbital ecchymosis, indicating anterior fossa involvement
- Haemotympanum — blood visible behind the tympanic membrane
- CSF rhinorrhoea or otorrhoea — leakage of CSF; confirmed by glucose on dipstick or beta-2 transferrin assay
Mass Effect and Herniation
Mass effect refers to displacement of normal brain structures by an expanding intracranial lesion. In TBI, mass effect from an expanding haematoma or diffuse cerebral swelling is a direct cause of secondary brain injury and death — it is not the primary injury itself but rather its consequence.
CT Signs of Mass Effect
- Midline shift: Displacement of the septum pellucidum from midline. Measured at the level of the septum. Shift >5 mm is clinically significant; >10 mm often indicates urgent surgical need.
- Sulcal effacement: Loss of cortical sulci as swollen brain presses against the inner skull
- Ventricular compression: Ipsilateral lateral ventricle becomes slit-like; contralateral ventricle may dilate (trapped)
- Cisternal effacement: Loss of normal CSF-density basal cisterns — a critical sign indicating impending herniation
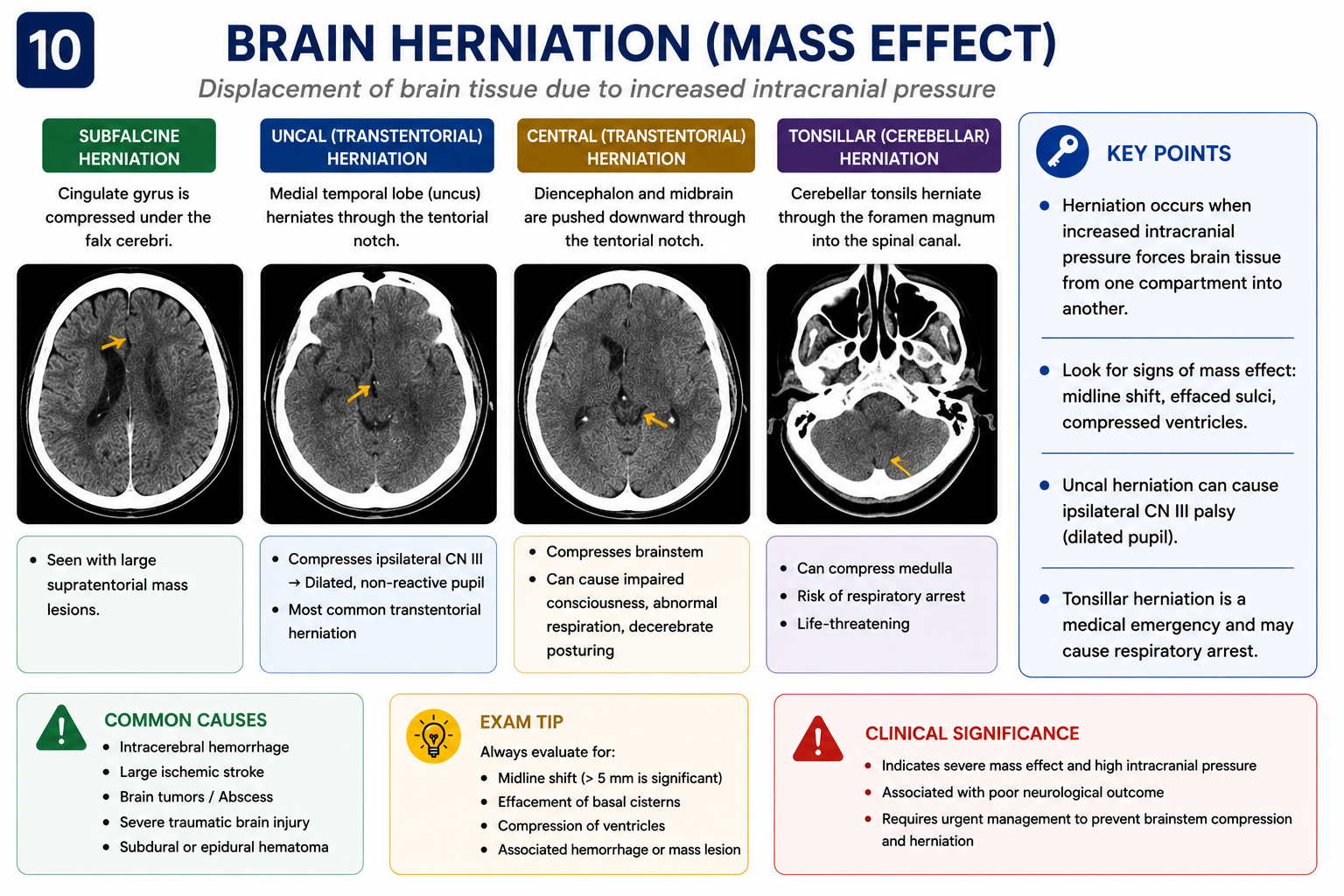
Herniation Syndromes
| Type | Description | Clinical Features |
|---|---|---|
| Uncal (transtentorial) | Medial temporal lobe herniates through the tentorial notch | Ipsilateral fixed dilated pupil (CN III compression), contralateral hemiplegia, progressive coma |
| Central transtentorial | Bilateral downward herniation through tentorial notch | Bilateral small pupils, progressive coma, Cheyne-Stokes respiration |
| Tonsillar (coning) | Cerebellar tonsils herniate through foramen magnum | Cushing's response (bradycardia + hypertension), apnoea, death |
| Subfalcine | Cingulate gyrus herniates under the falx | Often initially asymptomatic; may compromise anterior cerebral artery territory |
Effacement of the basal cisterns (perimesencephalic, suprasellar, or quadrigeminal plate) is one of the most critical CT findings in TBI. It indicates severely raised ICP with impending herniation and demands immediate neurosurgical involvement. Bilateral cisternal effacement carries a very poor prognosis.
How to Present and Report Trauma CT Findings
Recognising a CT abnormality is only part of the task. Medical students and junior doctors should also be able to describe findings in a structured and clinically useful way. A good trauma CT presentation identifies the location, density, shape, size, associated mass effect, and any urgent neurosurgical concerns.
General Reporting Structure
- Identify the compartment involved (extra-axial vs intra-axial; which space)
- Describe the density (hyperdense, isodense, hypodense, mixed)
- Describe the shape and distribution (biconvex, crescent, focal, diffuse)
- Estimate size where possible (maximum thickness in mm)
- Assess for mass effect (sulcal effacement, ventricular compression)
- Comment on midline shift (measured at the septum pellucidum, in mm)
- Assess ventricles and basal cisterns (open, compressed, asymmetric)
- Comment on fractures (type, location, relationship to vascular structures)
- State the likely diagnosis
- Mention any urgent findings requiring immediate action
Example Reports
"Large right temporal acute epidural haematoma. Hyperdense biconvex extra-axial collection measuring approximately 18 mm in maximum thickness. Associated right temporal bone fracture. Significant local mass effect with compression of the ipsilateral lateral ventricle and approximately 8 mm midline shift to the left. Appearance consistent with an acute epidural haematoma requiring urgent neurosurgical review."
"Acute left frontoparietal subdural haematoma. Crescent-shaped hyperdense extra-axial collection crossing suture lines. Associated sulcal effacement and approximately 5 mm midline shift to the right. Underlying cerebral oedema is present."
"Hyperdense blood is present within the right Sylvian fissure and adjacent cortical sulci. Findings are consistent with traumatic subarachnoid haemorrhage. No significant mass effect. Basal cisterns are open."
"Multiple haemorrhagic contusions involving the bilateral frontal lobes. Heterogeneous hyperdense and hypodense areas consistent with haemorrhagic contusions. Associated surrounding vasogenic oedema and mild local mass effect. Serial CT recommended to monitor for haemorrhagic progression."
Post-Traumatic Hydrocephalus
Hydrocephalus is abnormal accumulation of CSF within the ventricular system. In TBI, the most common cause is blood in the subarachnoid space impairing CSF reabsorption at the arachnoid granulations (communicating hydrocephalus). Direct obstruction of CSF flow pathways by blood clot or oedema causes obstructive (non-communicating) hydrocephalus.
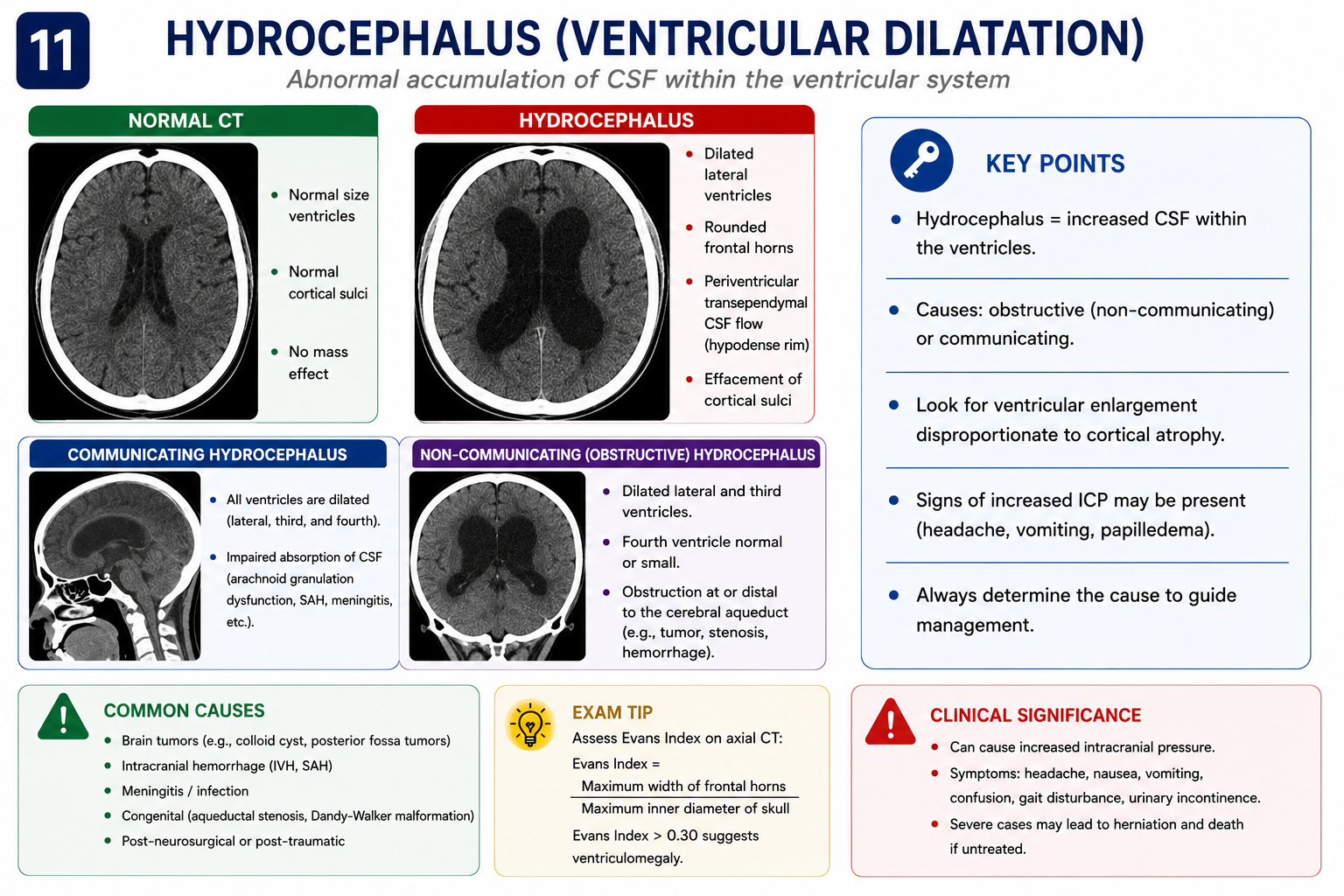
CT Features of Hydrocephalus
- Ventricular enlargement disproportionate to any cerebral atrophy
- Temporal horn rounding — temporal horns become rounded and enlarged (normally they are slit-like)
- Periventricular low attenuation ("halo") — hypodense rim around ventricles representing transependymal CSF flow under pressure
- Sulcal effacement — in contrast to atrophic dilatation, where sulci are widened
Hydrocephalus vs cerebral atrophy: Both cause ventriculomegaly. In atrophy, sulci are widened and periventricular oedema is absent. In hydrocephalus, sulci are effaced (or normal), and periventricular lucency may be present. Atrophy is a loss of brain tissue; hydrocephalus is a pressure-driven process — they require different management.
Pneumocephalus
Pneumocephalus is the presence of air within the cranial vault. In trauma, it occurs when a fracture creates a communication between an air-containing space (paranasal sinuses, mastoid air cells, or nasal cavity) and the intracranial compartment, indicating disruption of the dural barrier.
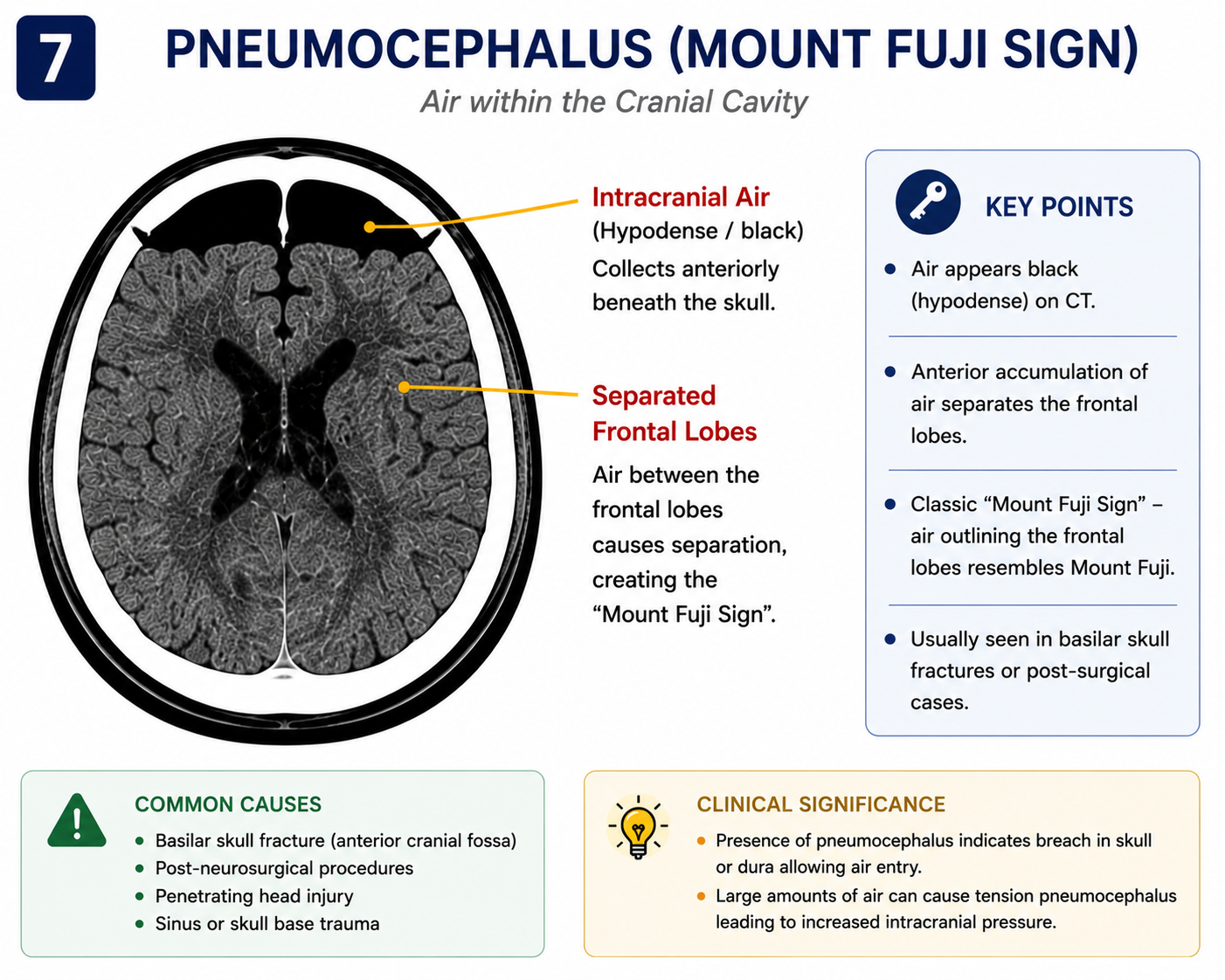
CT Appearance
- Air is the most hypodense substance on CT (~−1000 HU) — appears jet black
- Seen as black collections within the cranial vault, ventricles, or subarachnoid space
- Small amounts are common after skull base fractures and are clinically insignificant
Tension Pneumocephalus
Tension pneumocephalus occurs when air accumulates under pressure, producing mass effect. The Mount Fuji sign — bilateral frontal air collections causing compression and anterior separation of the frontal lobes, resembling the outline of Mount Fuji — is the CT hallmark of tension pneumocephalus and requires urgent neurosurgical decompression.
All patients with traumatic pneumocephalus have a disrupted dural barrier and are at risk of ascending meningitis. Assess for CSF leak (rhinorrhoea or otorrhoea). Simple pneumocephalus usually resolves with 100% oxygen therapy (accelerates air resorption); tension pneumocephalus requires needle decompression or formal surgery.
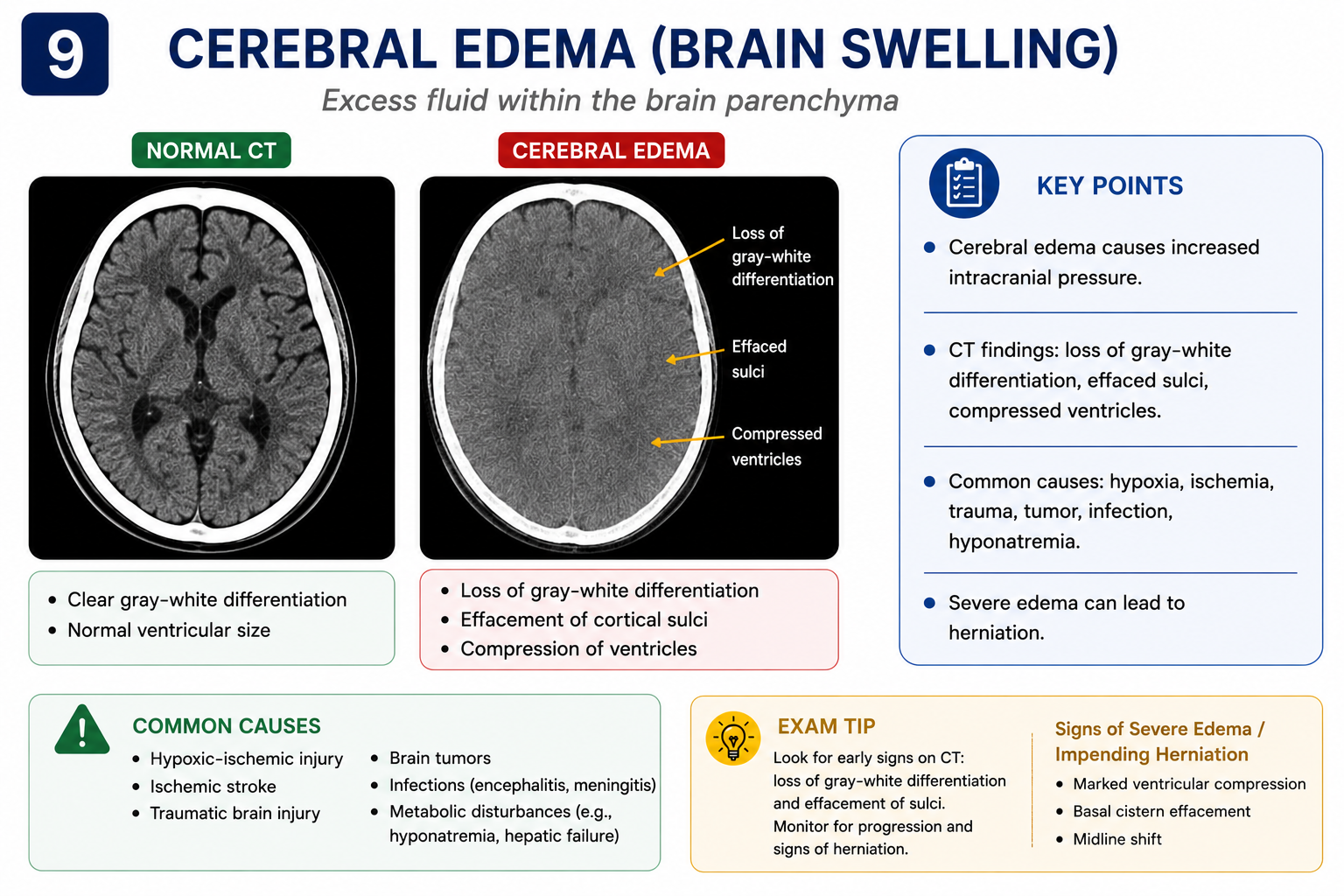
Cerebral Oedema
Cerebral oedema is an increase in brain water content leading to brain swelling. In TBI it can be focal (surrounding a contusion or haematoma) or diffuse (affecting the entire brain). Diffuse cerebral oedema is a life-threatening complication of severe TBI, particularly in children.
| Type | Mechanism | Common Cause | CT Appearance |
|---|---|---|---|
| Cytotoxic | Na/K ATPase failure → intracellular swelling | Ischaemia, hypoxia, severe TBI | Loss of grey–white differentiation; gyral swelling |
| Vasogenic | Blood–brain barrier breakdown → extracellular oedema | Contusions, haematomas, tumours | Hypodensity in white matter, finger-like projections |
| Interstitial | Transependymal CSF flow | Hydrocephalus | Periventricular hypodense halo |
CT Signs of Diffuse Cerebral Oedema
- Loss of grey–white differentiation — normally grey matter is slightly denser; this distinction is obliterated in diffuse oedema
- Diffuse sulcal effacement — gyri press against the skull
- Cisternal effacement — basal cisterns become compressed or invisible
- Slit ventricles — compressed by surrounding swollen brain
- Reversal sign (severe cases) — grey matter appears hypodense relative to white matter; indicates severe diffuse hypoxic–ischaemic injury with very poor prognosis
Diffuse cerebral swelling is more common and more severe in children than adults, partly due to immature cerebrovascular autoregulation. In infants with bilateral SDH and diffuse oedema without a clear accidental trauma mechanism, non-accidental injury (NAI) must be considered and appropriate safeguarding protocols followed.
Summary — Key CT Findings in TBI
- CT density: Acute blood is hyperdense; oedema and CSF are hypodense; air is very hypodense (black)
- EDH: Biconvex hyperdense collection; does not cross sutures; temporal most common; middle meningeal artery
- SDH: Crescent-shaped; crosses sutures; density changes with age — acute (hyper) → subacute (iso) → chronic (hypo)
- Traumatic SAH: Hyperdense blood in sulci and cisterns; can cause communicating hydrocephalus
- Contusions/ICH: Frontal and temporal poles; coup-contrecoup; may blossom on serial CT
- Skull fractures: Always review bone windows; basilar fractures risk CSF leak and meningitis
- DAI: Shearing injury; CT may be normal despite severe neurological deficit; MRI SWI is most sensitive
- Mass effect: Midline shift, sulcal effacement, cisternal compression — urgent if >5 mm shift or basal cistern obliteration
- Reporting: Location, density, shape, size, mass effect, midline shift, cisterns, fractures, diagnosis, urgent findings
- Hydrocephalus: Temporal horn rounding, periventricular lucency; distinguish from atrophy
- Pneumocephalus: Black air in cranial vault; Mount Fuji sign = tension pneumocephalus
- Cerebral oedema: Loss of grey–white differentiation, slit ventricles, absent basal cisterns
- CT windows: Brain window for haemorrhage; bone window for fractures; subdural window for isodense collections
Common Exam Points
- EDH shape: "Biconvex" is the keyword. Does not cross sutures. Middle meningeal artery at pterion.
- SDH vs EDH: Crescent vs biconvex is the classic exam distinction.
- Isodense SDH: Subacute (day 3–21). Look for indirect signs: sulcal asymmetry, displaced cortical margin, midline shift.
- Lucid interval: Classic for EDH but occurs in a minority — its absence does not exclude the diagnosis.
- Thunderclap headache: Treat as spontaneous SAH until proven otherwise — even if CT is negative, LP or CT angiography is required.
- Frontal/temporal poles: Classic locations for cerebral contusions due to coup-contrecoup mechanism.
- Contusion blossoming: Always warn about haemorrhagic progression on serial CT — a key management point.
- NICE head injury CT indications (adults): GCS <13 on first assessment; suspected open, depressed, or basilar skull fracture; post-traumatic seizure; focal neurological deficit; ≥2 vomiting episodes; amnesia >30 min of events before injury.
- Basal cistern effacement: Critical sign of raised ICP — requires immediate neurosurgical involvement.
- Mount Fuji sign: Bilateral frontal air with frontal lobe separation = tension pneumocephalus = neurosurgical emergency.
Frequently Asked Questions
References and Suggested Reading
- National Institute for Health and Care Excellence (NICE). Head injury: assessment and early management. Clinical Guideline NG232. London: NICE; 2023.
- Broder J. Diagnostic Imaging for the Emergency Physician. Philadelphia: Elsevier Saunders; 2011.
- Wintermark M, Sanelli PC, Anzai Y, et al. Imaging evidence and recommendations for traumatic brain injury. AJNR Am J Neuroradiol. 2015;36(2):E1–E11.
- Osborn AG. Osborn's Brain: Imaging, Pathology and Anatomy. 2nd ed. Philadelphia: Elsevier; 2018.
- Gean AD. Brain Injury: Applications from War and Terrorism. Philadelphia: Wolters Kluwer; 2014.
- Smits M, Dippel DW, de Haan GG, et al. External validation of the Canadian CT Head Rule and the New Orleans Criteria for CT scanning in patients with minor head injury. JAMA. 2005;294(12):1519–1525.
- Advanced Trauma Life Support (ATLS) Student Course Manual, 10th edition. American College of Surgeons, 2018.
- Radiopaedia.org — CT head atlas and case-based radiology learning
- NICE Guideline NG232 — Head injury: assessment and early management (2023)
- ATLS 10th Edition — Head Trauma chapter
- Osborn's Brain (2nd ed) — Reference text for neuroradiology
This article is intended for medical education only. It is designed for medical students, intern doctors, and junior doctors and does not constitute clinical advice. Always refer to current local guidelines, senior clinical input, and specialist radiology opinion when interpreting CT scans and managing patients. CT interpretation in clinical practice requires formal training and should be performed in the appropriate clinical context.
- CT Density Basics
- CT Window Settings
- Systematic Approach
- Normal CT Anatomy
- Epidural Haematoma
- Subdural Haematoma
- Subarachnoid Haemorrhage
- ICH & Contusions
- Diffuse Axonal Injury
- Skull Fractures
- Mass Effect & Herniation
- How to Report Findings
- Complications
- Hydrocephalus
- Pneumocephalus
- Cerebral Oedema
- Summary
- Exam Points
- FAQ
- References